OCD Demystified: Types, Symptoms & What’s Not OCD
|
15
min read
|
Tanvi

OCD Is Not What You Think It Is
OCD isn’t a personality quirk. It’s not about being “extra clean” or “super organized”. And no, it’s not something to casually joke about in memes or movies.
Obsessive-Compulsive Disorder (OCD) is a serious and often misunderstood mental health condition that affects how people think, feel, and behave. For someone living with OCD, it’s not about liking things neat - it’s about battling relentless thoughts and performing exhausting rituals just to feel okay.
In India, OCD affects an estimated 0.8% of the population, according to a study by Jaisoorya et al. That may sound small, but it translates to millions of people silently struggling, often mislabelled as “fussy” or “overly sensitive” by friends, families, and even workplaces.
The truth is, OCD can severely impact daily life - interfering with work, relationships, sleep, and self-worth. But here’s the good news: with proper diagnosis and the right therapeutic support, OCD is treatable. And thanks to platforms like Elfina, that help can now be accessed online, discreetly, safely, and on your terms.
What Is OCD? Breaking It Down Simply
Obsessive-Compulsive Disorder (OCD) is a mental health condition marked by two main components:
Obsessions: These are intrusive, unwanted thoughts, images, or urges that cause distress, anxiety, or fear. They aren’t simply worries - they feel uncontrollable and deeply disturbing.
Compulsions: These are repetitive behaviors or mental actions performed to try and neutralize the anxiety caused by the obsessions. The relief is temporary, but the cycle repeats.
According to the American Psychological Association (APA), these cycles can become so time-consuming and emotionally exhausting that they interfere with daily activities - from brushing your teeth to attending work.
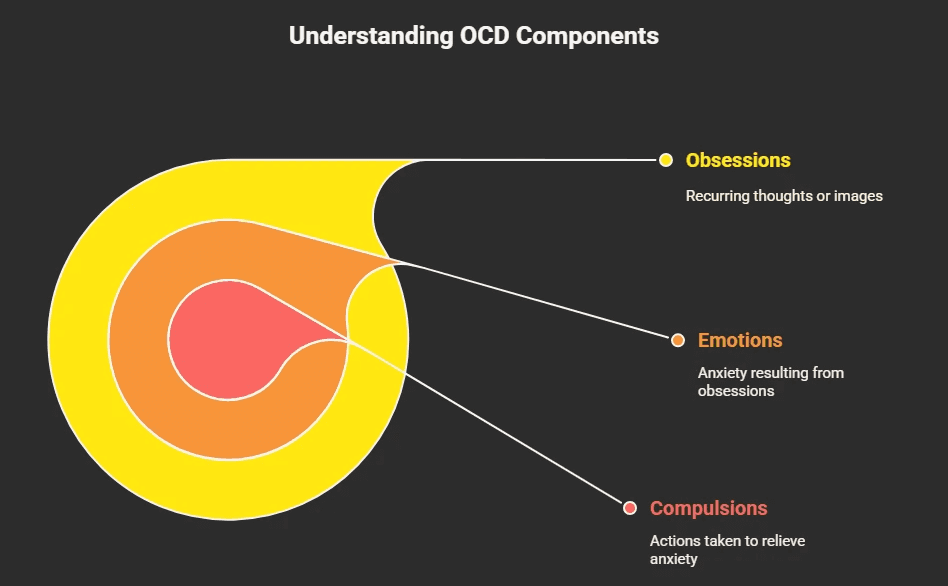
The NHS breaks OCD into three parts:
Obsessions: The thought - “Did I lock the door?”
Emotions: The resulting anxiety - “What if someone breaks in?”
Compulsions: The action - checking the lock 15 times to calm the fear.
Importantly, the person knows the obsession may not make sense - but the fear still feels real, and the compulsion feels necessary.
Obsessions vs. Compulsions: Real-World Examples That Hit Home
OCD doesn’t look the same for everyone - and it’s not always visible. Here's how the cycle often plays out:
Obsessions (Intrusive Thoughts or Urges):
Contamination fears:
“What if I touched something germy and brought illness home?”Violent intrusive thoughts:
“What if I suddenly lose control and hurt someone I care about?”Religious/guilt-based obsessions:
“What if I blasphemed or committed a sin without realizing it?”Sexual or identity-related thoughts:
“What if I’m sexually attracted to someone I shouldn’t be?”
(OCD UK highlights that the brain is powerful enough to trigger physical responses even to intrusive and distressing thoughts - especially in OCD themes around sexuality - making the fear feel intensely real and deeply confusing.)
These thoughts aren’t wishes. In fact, they’re the opposite - they go against a person’s values, which is what makes them so upsetting.
Compulsions (Actions or Mental Rituals to Neutralize the Thought):
Handwashing or cleaning: Over and over until it “feels right”.
Checking: Doors, gas knobs, appliances - again and again.
Mental rituals: Silently counting, praying, repeating phrases.
Avoidance: Skipping entire locations, people, or tasks out of fear of triggering obsessions.
While these behaviors may bring brief relief, they also reinforce the anxiety loop, making the OCD stronger over time.
Compulsions vs. Rituals: There’s a Subtle But Crucial Difference
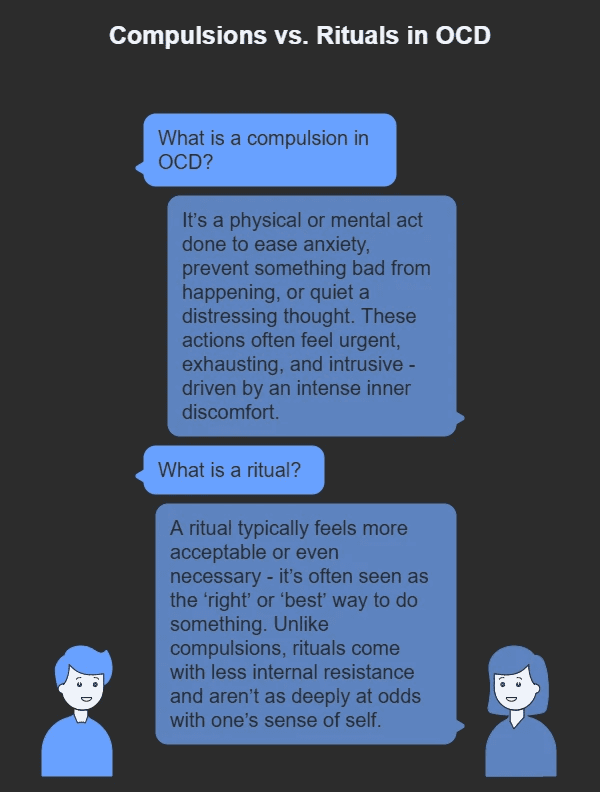
The terms compulsions and rituals are often used interchangeably - and that makes sense, because in OCD, compulsions often take the form of ritualistic behavior. But as the International OCD Foundation clarifies, “not all repetitive behaviors or ‘rituals’ are compulsions”. Understanding the difference is key to identifying OCD and providing the right treatment.
A compulsion in OCD is an action (physical or mental) that’s performed to reduce anxiety, prevent harm, or neutralize a disturbing thought. These are typically unwanted, exhausting, and feel urgent. They’re driven by internal distress - not desire.
A ritual, however, while it may look similar on the outside (like repeated cleaning or checking), often comes with less internal resistance. In fact, rituals might be perceived by the person as the right or best way to do something. They are less “ego-dystonic”, meaning they don’t clash as painfully with the person’s own values or self-image.
For instance, a person might believe that a surface isn’t truly clean unless it’s scrubbed in a very particular sequence - and if the order is broken, they may feel compelled to start over. In such cases, the ritual might feel justified, even if it's time-consuming.
That said, not all compulsions are rituals - and not all rituals are compulsions. If someone showers excessively, but doesn’t follow a fixed sequence, it may not be ritualized. On the other hand, a ritual with a strict, repeated pattern - one that aims to reduce a fear or avert a specific outcome - could very well be a compulsion.
In essence:
Compulsions are driven by anxiety and performed to relieve it.
Rituals may be perceived as necessary or “correct” rather than distress-driven.
Many compulsions are ritualized, but not all rituals are compulsive.
The difference lies in the underlying drive - whether it’s anxiety and fear, or a rigid sense of “rightness”.
Inside the Mind: Key Characteristics of OCD
OCD isn’t just about being "extra neat" or "a bit anxious". At its core, it's a tangled loop of distress, doubt, and ritual - one that people don't choose, and often desperately want to break.
One key feature of OCD is that it’s ego-dystonic. That’s a fancy way of saying the thoughts and urges don’t align with who you are. They feel intrusive, distressing, and completely out of character. Imagine your mind sending you signals that go against your deepest values - that’s what ego-dystonic means. A person might have violent thoughts but feel horrified by them. Or they might be obsessing about harming someone they love, despite having no desire to do so.
This inner tug-of-war causes intense anxiety, which fuels the next phase: compulsions. These are actions - like checking, cleaning, or repeating - done to get relief. But it’s temporary. The anxiety creeps back in, and the cycle starts again.
Anxiety → Compulsion → Temporary relief → Anxiety again.
Interestingly, many adults with OCD know their behaviors don’t make logical sense, as the National Institute of Mental Health (NIMH) notes. Yet, they still feel trapped in performing them, because the fear of something terrible happening is overwhelming. It also mentions how children often lack the insight to recognize these rituals as irrational - they just know something bad might happen if they don’t comply.
This push-pull dynamic often leads to rumination - the mental replay button that never stops. It’s not just overthinking. Rumination is a vulnerability factor, a kind of cognitive trap that keeps feeding the OCD cycle. People get stuck analyzing their thoughts or actions endlessly, searching for certainty - and never finding it.
OCD isn't just a quirk. It's a deeply distressing condition where your own mind becomes the source of fear - and your actions, a desperate attempt to feel safe.
Symptoms of OCD: When Thoughts Take the Driver’s Seat
Everyone gets weird thoughts sometimes. But for someone with OCD, these thoughts don’t just pass through - they take the wheel, grip tight, and refuse to let go.
Obsessions are the starting point. These are not your everyday worries - they’re intrusive, persistent, and disturbing. They're not wanted, and they don’t feel good. The distress they cause can disrupt everything - sleep, work, relationships.
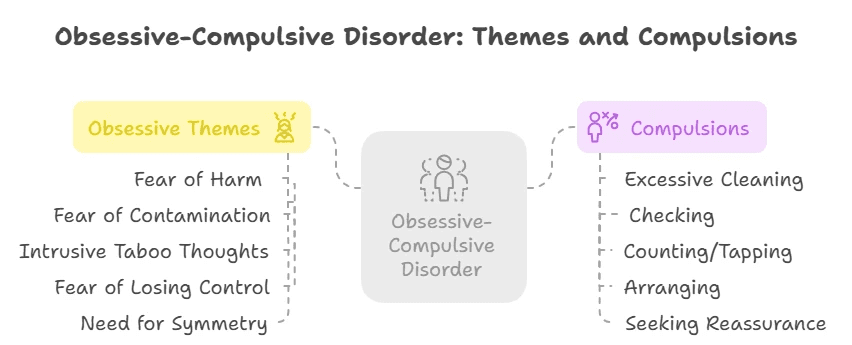
Some common obsessive themes include:
Fear of harm or causing harm, even accidentally
Fear of contamination or illness - germs, dirt, bodily fluids
Intrusive taboo thoughts - involving violence, sex, or religion
Fear of losing control - like shouting something offensive or doing something impulsive
A need for things to feel 'just right' or symmetrical
Then come the compulsions - the brain's attempt to neutralize those distressing thoughts:
Excessive cleaning/washing until skin is raw
Checking - doors, locks, stoves - again and again
Counting, tapping, or repeating specific actions a certain number of times
Arranging things until they’re “perfect”
Seeking constant reassurance, from loved ones or even Google
It's not the presence of these thoughts alone that defines OCD, but the distress and disruption they cause. If the thoughts or behaviors are affecting your quality of life, it’s more than a personality quirk - it’s a mental health condition.
And you’re not alone. OCD is treatable, and help is out there.
Decoding OCD: A Deep Dive into Common Subtypes
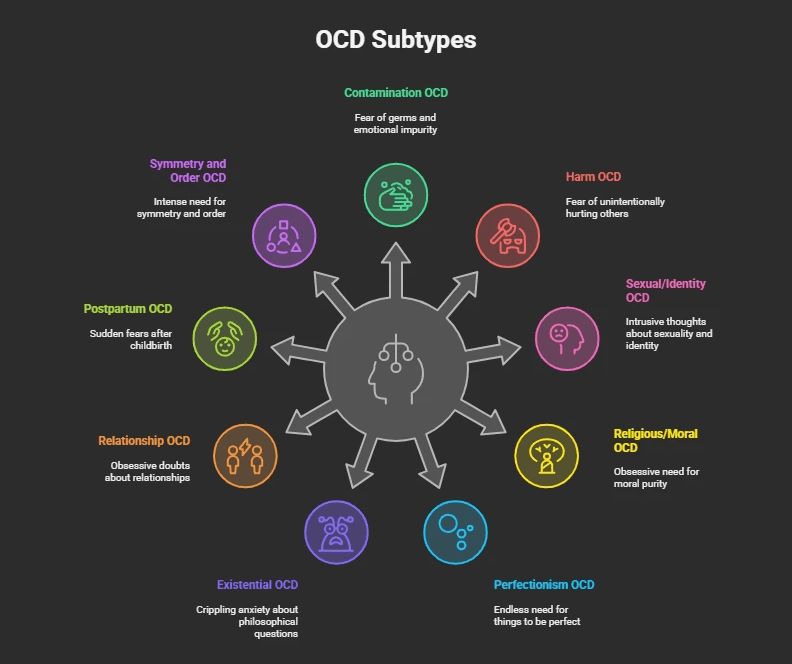
OCD is a shapeshifter - it doesn’t always look the same for everyone. While the underlying mechanism is the same (obsession + compulsion), the themes and triggers can differ wildly. Let’s explore the most common OCD subtypes:
1. Contamination OCD
The classic germ-fear. But it’s more than just being tidy - it’s a paralyzing fear of dirt, disease, or even emotional “contamination”. Some fear that touching certain people or objects might make them morally impure or absorb unwanted traits.
2. Harm OCD
Terrified of hurting someone - not because you want to, but because you’re scared you might. These thoughts are ego-dystonic, meaning they feel completely wrong. Still, the fear persists: “What if I snap?”
3. Sexual/Identity OCD (HOCD, POCD, ROCD)
These involve intrusive thoughts about sexuality, children, or relationships that clash painfully with the person's identity or values. More on this in the next section.
4. Religious/Moral OCD (Scrupulosity)
A consuming need to be morally or spiritually “pure”. People may pray repeatedly, seek forgiveness obsessively, or worry they’ve committed blasphemy.
5. Perfectionism OCD
Not just “wanting things neat” - this subtype drives people to endlessly redo tasks until they’re “just right,” often at the cost of time, relationships, and peace.
6. Existential OCD
Imagine your brain stuck on questions like “Why are we here?” or “What if none of this is real?” - not for curiosity, but from crippling anxiety. These philosophical spirals are endless and distressing, often leading to a deep sense of disconnection or dread.
7. Relationship OCD (ROCD)
People with ROCD obsess over whether their partner is "the one," if they feel enough love, or if a past relationship was better. They may check their feelings repeatedly, compare partners, or seek reassurance - all while feeling more confused and isolated.
8. Postpartum OCD
Unlike typical OCD, this form can emerge suddenly after childbirth, with terrifying thoughts of harming the baby or being a bad parent. It's not a sign of intent - it's a mental health condition, and treatable.
9. Symmetry and Order OCD
A powerful need for symmetry or things to be “just so”. People may spend hours arranging objects, redoing tasks, or feeling intense discomfort if something is out of place.
OCD can wear many masks - but no matter the subtype, you’re not alone, and your experience is valid.
HOCD, POCD, ROCD & OCD Spikes: The OCD Experience No One Talks About
These lesser-known OCD subtypes often come with deep shame, misunderstanding, and silence. But naming them is the first step to healing.
HOCD (Homosexual OCD or Sexual Orientation OCD)
This involves obsessive fears of being gay when you're straight - or vice versa. It's not about homophobia or confusion, but a relentless need for certainty. Every gesture, thought, or glance can feel like a sign - triggering panic. People may compulsively check their arousal, avoid same-sex individuals, or replay interactions mentally.
POCD (Pedophilia OCD)
One of the most distressing forms. People with POCD experience unwanted, intrusive thoughts about children - not because they desire them, but because they are terrified by them. These thoughts cause overwhelming guilt and shame, leading to compulsive behaviors like avoiding children, seeking reassurance, or checking their own feelings repeatedly.
ROCD (Relationship OCD)
Obsessions about romantic partners. “Do I really love them?” “What if they’re not right for me?” “What if I’m settling?” These aren’t just cold feet - they’re obsessive doubts, often followed by compulsions like comparing, analyzing, visualizing happy scenarios, or asking for constant validation.
OCD Spikes
As described by OCD UK, “spikes” generally refer to sudden, intense waves of distress triggered by an obsession. It’s like a mental ambush - out of nowhere, a thought grabs you, and the anxiety skyrockets. The spike includes the trigger, the obsession itself, and the distress that follows.
These spikes can feel like emotional whiplash. One moment you're fine, the next you’re overwhelmed, desperate for reassurance, and stuck in the OCD cycle again.
Each of these subtypes reflects the same underlying problem: intrusive thoughts + anxiety + compulsions. But because these themes are so misunderstood, many suffer in silence.
You are not your thoughts. OCD is lying to you - but support, therapy, and compassion can help you take your mind back.
“Obsessed” vs OCD: It’s Not What You Think
We’ve all heard phrases like “I’m so OCD about my desk!” or “She’s obsessed with that show!” - but there’s a world of difference between being passionate or particular and actually living with Obsessive-Compulsive Disorder (OCD).
OCD is not about enjoying routines, being tidy, or liking things a certain way. It's about intrusive, unwanted thoughts (obsessions) that trigger intense anxiety, and repetitive actions (compulsions) meant to neutralize that anxiety. These compulsions don’t bring satisfaction - only temporary relief, if any.
Think of it this way: passion drives you forward, OCD holds you hostage.
Let’s bust another myth while we’re at it:
OCD ≠ OCPD (Obsessive-Compulsive Personality Disorder).
As Rizvi A. and Torrico TJ explain in their book Obsessive-Compulsive Personality Disorder, OCD is defined by ego-dystonic experiences - people don’t want these thoughts or behaviors. They're distressing and feel alien. In contrast, OCPD traits are ego-syntonic - a person sees their need for control, order, and perfectionism as right, even if it creates friction with others.

So the next time someone says they’re “so OCD” because they like a neat planner or a spotless kitchen, it’s worth remembering: OCD isn’t about preference. It’s about persistent mental torment that most people would do anything to silence.
What Causes OCD? The Puzzle Pieces Behind the Disorder
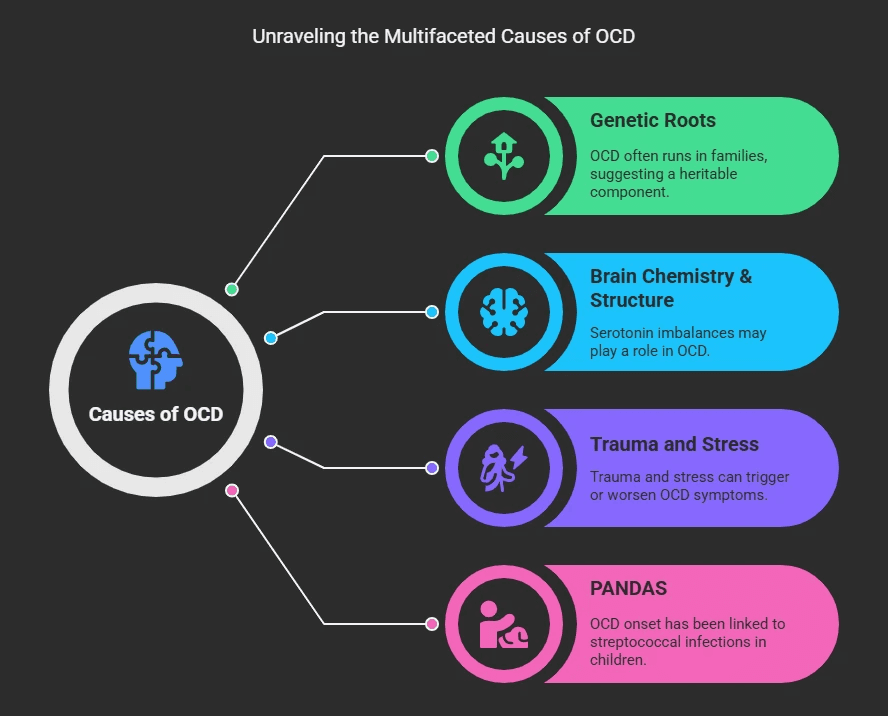
OCD doesn’t have a single cause - it’s more like a puzzle made up of biology, life experiences, and even ancient bacteria.
Genetic Roots: Research shows that OCD often runs in families. Twin and family studies suggest that certain forms of OCD have a heritable component, meaning if a close relative has it, the risk increases.
Brain Chemistry & Structure: Some theories point to abnormalities in serotonin levels - a brain chemical involved in mood and behavior regulation. While it’s unclear whether this imbalance causes OCD or is an effect of it, it's a key area of focus in treatment.
Trauma and Stress: A history of trauma or intense stress can trigger or worsen OCD symptoms. The brain sometimes responds to trauma by trying to create “safety” through compulsive rituals or thoughts.
PANDAS: When Strep Affects the Mind
In children, a rapid onset of OCD symptoms can be linked to PANDAS (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections). Imagine waking up one day and your child is suddenly performing compulsive rituals, battling tics, or panicking about being apart from you.
Here’s why: Strep bacteria are sneaky. Through a process called molecular mimicry, they disguise themselves to look like healthy brain tissue. But once the immune system fights back, it may accidentally attack parts of the brain too - particularly those linked to behavior and emotion.
While PANDAS is still under investigation, its dramatic onset and symptoms are a reminder that OCD can be more than just psychological - it can be immunological.
Who’s at Risk? Understanding OCD’s Contributing Factors
OCD doesn’t discriminate - it affects people across all ages, genders, and cultures. But some factors can increase your likelihood of developing it:
Family History: If a parent, sibling, or close relative has OCD or an anxiety disorder, your risk goes up. Genetics play a key role, even if they’re not the full story.
Childhood Trauma: Experiencing neglect; emotional, physical, or sexual abuse - especially during formative years - can be a major trigger. The brain may learn to associate certain thoughts or actions with protection or safety.
Major Life Stressors: Moving, divorce, losing a loved one, or starting a new job or school - these stress points can all provoke OCD symptoms, particularly if they come on suddenly or are difficult to process emotionally.
Other Mental Health Conditions: OCD often coexists with anxiety disorders, depression, and sometimes ADHD or tic disorders. It’s not rare for individuals to navigate multiple mental health conditions at once.
Think of these factors as fuel - they don’t guarantee the fire of OCD will start, but under the right conditions, they can fan the flames.
Related Disorders: When It’s Not Just OCD
OCD often overlaps with or gets confused with other conditions that involve compulsions, obsessions, or body-focused repetitive behaviors. Understanding the differences can lead to better care.
Body Dysmorphic Disorder (BDD)
Both BDD and OCD involve repetitive checking. But in BDD, the obsession centers exclusively on appearance. Individuals may fixate on perceived flaws, often seeking cosmetic procedures. People with OCD don’t usually have thoughts or rituals linked to their looks.
Trichotillomania (Hair Pulling)
This isn’t about “playing with your hair” - it’s a clinical disorder. To be diagnosed, the person must have repeated hair pulling that leads to noticeable hair loss, feel unable to stop, and experience significant distress or disruption. The APA clarifies that it must not be due to a medical or another mental condition.
Excoriation Disorder (Skin Picking)
Similar to trichotillomania, but the focus is on skin. People pick at real or perceived blemishes, often to the point of injury or infection. It’s not a simple habit - it’s compulsive and emotionally distressing.
Tic Disorders & GAD
Tics (sudden, repetitive movements or sounds) and Generalized Anxiety Disorder (GAD) may co-occur with OCD. While GAD involves persistent worrying, OCD is more specific - compulsions arise from intrusive thoughts that demand neutralization.
Each of these conditions is unique, but they share a thread: repetitive thoughts or actions that interfere with daily life. Understanding their nuances matters.
Postpartum OCD: The Silent Struggle After Birth

We often hear about Postpartum Depression, but what if your mind suddenly floods with terrifying thoughts of harming your baby - and you’re horrified by them?
This is Postpartum OCD, and it’s more common than most people think. It typically emerges shortly after childbirth and involves disturbing, unwanted thoughts (obsessions) - often about harming the baby - even though the parent would never actually do so. To reduce the anxiety caused by these thoughts, they may develop compulsions, like checking locks, avoiding the baby, or cleaning excessively.
These thoughts are not psychotic hallucinations. People with Postpartum OCD know the thoughts are irrational and upsetting. That’s what makes it so distressing - they feel out of control, but they’re fully aware.
What’s more, fathers can experience it too, as highlighted by the Postpartum Depression Org. Dads may also have intrusive thoughts or compulsions related to their child’s safety and their own parenting.
This condition is often mistaken for Postpartum Depression or Psychosis, but it’s a different experience altogether. And because of the shame attached, many parents suffer in silence.
Postpartum OCD needs specialized, compassionate care - not judgment. With therapy, particularly CBT and Exposure and Response Prevention (ERP), many parents recover and bond healthily with their baby again.
OCD in Children: When OCD Comes Out of the Blue
We’ve touched on this earlier while discussing PANDAS - a rare but eye-opening condition where a simple strep throat could flip a child’s world upside down. To recap:
PANDAS stands for Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections. It’s when OCD or tics suddenly emerge or worsen dramatically after a strep infection, often “overnight and out of the blue”. These children may develop motor or vocal tics, intense obsessions or compulsions, anxiety, separation fears, and even mood swings.
This isn’t your usual gradual onset of OCD. It’s rapid, jarring, and deeply distressing - both for the child and their caregivers. Scientists believe this happens due to a case of molecular mimicry, where the immune system - in trying to fight the bacteria - mistakenly attacks parts of the child’s brain involved in behavior and emotion.
While research is still evolving, PANDAS highlights how OCD can manifest early and in deeply biological ways, sometimes without any psychological trigger at all.
Diagnosing OCD: What the DSM-5 Really Says
OCD isn’t diagnosed on a whim - it’s defined with precision. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5), issued by the American Psychiatric Association, outlines clear-cut criteria to ensure OCD is properly identified.
According to the DSM-5, OCD consists of:
Obsessions, which are:
Intrusive, unwanted thoughts, urges, or images that cause intense anxiety or distress.
The individual attempts to suppress or neutralize them (often by performing a compulsion).
Compulsions, which are:
Repetitive behaviors or mental rituals (like handwashing, counting, praying) that the person feels driven to perform to reduce their anxiety or prevent a feared event.
But these actions are not realistically connected to the feared event, or are clearly excessive.
Plus, to qualify as OCD:
These obsessions and/or compulsions must be time-consuming (typically more than 1 hour per day),
Or cause significant distress or impair the person’s social, occupational, or daily functioning.
This diagnostic clarity is critical. It draws the line between occasional worry or routine and a disorder that hijacks time, peace, and well-being.
Other Shades of OCD: When It Gets Complicated
OCD isn’t a static condition - it can shift, morph, and co-exist with other psychological states. Some features are less talked about, but they matter deeply.
🌩 Anxious Distress
It’s common, almost expected. But sometimes, this anxiety becomes chronic, intense, and deeply debilitating - fueling the obsessive-compulsive loop further.
🌑 Melancholy & Depression
Some individuals with OCD sink into melancholic depression, especially when compulsions feel inescapable or when obsessions attack core aspects of their identity.
🌀 Psychosis (Rare, But Real)
While rare, in some severe cases, OCD can be a precursor to psychotic symptoms. Obsessions might blend into delusional thinking, or the compulsions may take on bizarre, ritualistic qualities disconnected from logic or reality.
🌪 Mixed States: Mania + OCD
Occasionally, OCD overlaps with mania, especially in people with bipolar tendencies. This can result in erratic energy, hyper-focused compulsions, and intensified intrusive thoughts — making diagnosis and treatment more complex.
🔄 Rapid Cycling
Some experience obsessions and compulsions that evolve quickly, even within a single day or week - a storm of mental loops that rarely settles.
🤰 Hormones, Pregnancy & Seasonal Shifts
Pregnancy and hormonal changes can worsen OCD symptoms. Some individuals also report that OCD intensity varies with seasons, often flaring up during winter months.
Recognizing these layers helps demystify the rich and often challenging reality of living with OCD - a disorder that’s never one-size-fits-all.
Current Treatments for OCD
Here’s the hopeful part - OCD is treatable. The path isn’t always easy, but with the right combination of therapy, tools, and support, recovery is within reach.
🧠 Therapy is First-Line - and for Good Reason
Cognitive Behavioral Therapy (CBT): Rewiring the Thought Loop
Insert this YouTube Video: CBT for obsessive compulsive disorder (OCD)
CBT is a structured, skills-based approach that helps individuals recognize the patterns between obsessive thoughts, emotional distress, and compulsive behaviors. The goal? To interrupt the loop, reframe thoughts, and regain control.
CBT doesn’t ask people to ignore their distress. Instead, it equips them with tools to challenge distorted thinking, reduce avoidance, and respond to obsessions more rationally.
📊 In a controlled study of 40 individuals with OCD, 82.5% reported significant symptom improvement following CBT. Even more compelling: 57.5% achieved clinically significant results - a milestone that translates to real-life relief, not just better scores on paper.
CBT is especially effective when combined with ERP (Exposure and Response Prevention), which is often embedded within the CBT framework for OCD.
Exposure and Response Prevention (ERP): The Gold Standard
Insert this YouTube Video: ERP Therapy for OCD | A Complete Guide | #PaigePradko, #OCDwithPaige, #OCD
ERP is widely regarded as the gold standard for OCD treatment - and with good reason. It involves intentionally confronting feared thoughts or situations (exposure), while deliberately resisting the urge to perform compulsions (response prevention).
This process gradually helps the brain unlearn the association between obsessive thoughts and immediate danger.
But it’s not easy. The International OCD Foundation tells you to expect this when ERP is done properly:
You’ll initially feel more anxious, not less. Obsessions may spike. That’s a normal and expected part of the process.
You learn that these thoughts - while distressing - are not dangerous. The fear loses its grip.
Anxiety naturally fades over time as your brain habituates to the discomfort.
You reclaim confidence, learning that uncertainty can be tolerated, and that avoidance is not the only way to feel safe.
ERP changes how your brain processes fear and discomfort. It’s not about forcing yourself to be “okay” - it’s about learning to live without fear controlling your actions.
Acceptance and Commitment Therapy (ACT): Living with Meaning, Not Fear
Insert this YouTube Video: The OCD Mind and Uncertainty | ACT
ACT takes a slightly different approach. Rather than trying to eliminate intrusive thoughts, ACT helps individuals accept them as passing mental events, without judgment or over-identification.
The goal of ACT isn’t to suppress thoughts - but to shift your relationship to them. You learn to:
Allow distress to exist without acting on it.
Stop avoiding situations based on fear.
Live in alignment with your values, even if OCD symptoms persist in the background.
In a study by Soondrum, Tamini et al., ACT was found to significantly reduce OCD severity, with a large effect size on the YBOCS (Yale-Brown Obsessive Compulsive Scale) - a widely used clinical measure.
ACT can be especially effective for individuals with chronic OCD, those who’ve hit a wall with traditional methods, or anyone looking to improve overall quality of life alongside symptom relief.
🖥️ Online OCD Therapy with Elfina Therapists
You don’t need to sit in traffic or navigate waiting rooms to get life-changing OCD support. At Elfina, we bring evidence-based therapy directly to you - wherever you are.
Whether it’s ERP, CBT, or ACT, our expert clinicians are trained in the gold-standard treatments for OCD and tailor each session to your unique experience. Our therapists understand that OCD isn’t “one size fits all,” and neither is recovery. That’s why:
We match you with therapists who specialize in OCD - not generalists.
You’ll receive structured, science-backed care designed for your specific obsessions and compulsions.
We offer a private, judgment-free space where you can work through fears safely and openly.
Sessions are available online and on your schedule - because healing should work with your life, not against it.
With Elfina, therapy isn’t just convenient. It’s effective, accessible, and deeply personal.
💊 Medication
Often used alongside therapy, the NHS recommends SSRIs (Selective Serotonin Reuptake Inhibitors) as the first-line medication. They boost serotonin, a brain chemical involved in mood and anxiety.
It may take up to 12 weeks to see results, and like any medication, SSRIs can have side effects:
Feeling agitated or anxious
Nausea, dizziness, or headaches
Sleep issues or sexual side effects
🏡 Home Remedies & Self-Care That Actually Help
Journal your thoughts instead of acting on them. Let them exist on the page - not in your behavior.
Practice mindfulness - not just meditation, but grounding exercises, mindful walks, or sensory resets.
Reduce caffeine and stress - both amplify anxiety and compulsive urges.
Stick to routines and sleep schedules - stability helps the mind stay regulated.
💛 How to Support Someone with OCD
Watching someone you love struggle with OCD can feel overwhelming - but your support matters more than you know. Here’s how to show up with compassion and make a real difference.
1. Don’t Dismiss or Minimize Their Distress
OCD isn’t about “being dramatic” or “overthinking”. To the person experiencing it, their fears and compulsions feel very real. Avoid comments like “just relax” or “stop thinking about it” - these can unintentionally invalidate their experience.
Instead: Try, “That sounds really tough. I’m here for you.”
2. Don’t Enable – But Be Gentle
You may be tempted to help them avoid triggers or participate in rituals to reduce their anxiety - but this only reinforces OCD's grip.
Be supportive without feeding the cycle. If you're unsure how to navigate this, involve a therapist early on for guidance.
Try saying:
"I know this feels urgent right now. Would you like to try something we discussed in therapy instead?"
3. Be Patient with Their Recovery
OCD recovery isn’t linear. There will be progress, setbacks, victories, and relapses. Avoid rushing their healing or expecting “quick fixes”. Your consistent, non-judgmental presence is one of the best things you can offer.
4. Educate Yourself
Learn about OCD - not just the symptoms, but the science behind them. The more you understand, the more helpful and empathetic you can be.
Support doesn’t mean solving the problem. It means standing beside someone while they learn to solve it themselves.
🚫 What’s Not OCD
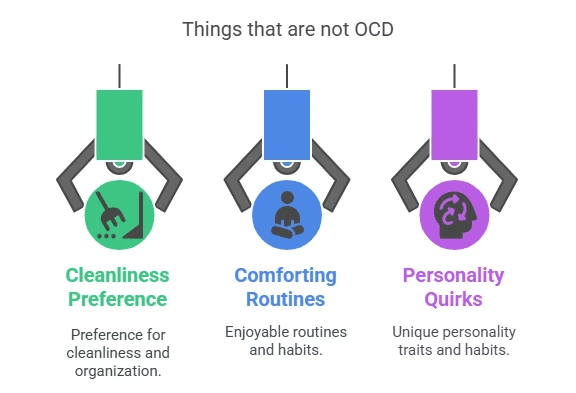
Let’s clear something up: OCD is not a personality trait, a joke, or a punchline. Misusing the term can minimize the lived experiences of people who struggle with it every day. Here’s what OCD isn’t:
❌ Liking Things Clean or Organized
Neatness or attention to detail isn’t the same as OCD.
A preference for clean spaces doesn’t involve distressing, repetitive thoughts or compulsive behaviors performed to reduce anxiety.
“I’m so OCD about my desk” is not only inaccurate - it’s dismissive.
❌ Having Routines or Quirks
Routines can be comforting. OCD compulsions, on the other hand, feel urgent and intrusive. They’re performed not out of habit, but out of a perceived need to prevent harm, discomfort, or catastrophe.
❌ A Quirky Personality Trait
OCD is a clinical diagnosis - a serious mental health condition. It involves real suffering and often interferes with relationships, careers, and daily functioning. Using "OCD" as slang only fuels misunderstanding and stigma.
Understanding what OCD isn’t helps us take what it is more seriously - and support those who need help more effectively.
🌐 Getting Diagnosed & Treated Online
Worried you might have OCD? Or maybe you’ve already been struggling in silence for years. Help is closer than you think.
At Elfina, we make expert OCD care available right from your home.

Here’s what makes Elfina’s online therapy stand out:
✔️ Evidence-Based Treatment
We use CBT, ERP, and ACT - the most effective, science-backed therapies for OCD. No fluff. Just proven methods that help you feel better.
🧠 Experienced OCD Specialists
Over 80% of our therapists have more than 5 years of experience treating complex conditions like OCD, anxiety, mood disorders, and burnout. You’re not getting a generalist - you’re getting a match who understands your specific needs.
⏱️ Flexible, Judgment-Free Support
You pick the time and place. Sessions are conducted online, so you can open up from wherever you feel safest.
🔒 Complete Privacy
Therapy should be safe in every sense. We offer a confidential, non-judgmental space to explore what’s going on inside your mind - and begin to untangle it with guidance and care.
🎯 94% of our clients find the right therapist on their first match - saving time, emotional energy, and unnecessary trial and error.
Conclusion: Your Path to Relief Starts Here
OCD can be isolating, overwhelming, and exhausting - but you don’t have to face it alone.
With the right tools, the right support, and the right therapy, relief is possible.
At Elfina, we understand OCD from both a clinical and human lens. Whether you’re just starting to question your symptoms or deep into your recovery journey, we’re here with:
Deep expertise in OCD and related disorders
Therapists who listen without judgment
Personalized treatment plans grounded in evidence
An online platform designed for comfort, flexibility, and long-term support
Your story with OCD doesn’t end at fear or frustration.
It can end at freedom.
Start your journey today - connect with an Elfina therapist who gets it.
Because better days aren’t just possible. With Elfina, they’re within reach. 💙


OCD Demystified: Types, Symptoms & What’s Not OCD
|
15
min read
|
Tanvi
OCD Is Not What You Think It Is
OCD isn’t a personality quirk. It’s not about being “extra clean” or “super organized”. And no, it’s not something to casually joke about in memes or movies.
Obsessive-Compulsive Disorder (OCD) is a serious and often misunderstood mental health condition that affects how people think, feel, and behave. For someone living with OCD, it’s not about liking things neat - it’s about battling relentless thoughts and performing exhausting rituals just to feel okay.
In India, OCD affects an estimated 0.8% of the population, according to a study by Jaisoorya et al. That may sound small, but it translates to millions of people silently struggling, often mislabelled as “fussy” or “overly sensitive” by friends, families, and even workplaces.
The truth is, OCD can severely impact daily life - interfering with work, relationships, sleep, and self-worth. But here’s the good news: with proper diagnosis and the right therapeutic support, OCD is treatable. And thanks to platforms like Elfina, that help can now be accessed online, discreetly, safely, and on your terms.
What Is OCD? Breaking It Down Simply
Obsessive-Compulsive Disorder (OCD) is a mental health condition marked by two main components:
Obsessions: These are intrusive, unwanted thoughts, images, or urges that cause distress, anxiety, or fear. They aren’t simply worries - they feel uncontrollable and deeply disturbing.
Compulsions: These are repetitive behaviors or mental actions performed to try and neutralize the anxiety caused by the obsessions. The relief is temporary, but the cycle repeats.
According to the American Psychological Association (APA), these cycles can become so time-consuming and emotionally exhausting that they interfere with daily activities - from brushing your teeth to attending work.
The NHS breaks OCD into three parts:
Obsessions: The thought - “Did I lock the door?”
Emotions: The resulting anxiety - “What if someone breaks in?”
Compulsions: The action - checking the lock 15 times to calm the fear.
Importantly, the person knows the obsession may not make sense - but the fear still feels real, and the compulsion feels necessary.
Obsessions vs. Compulsions: Real-World Examples That Hit Home
OCD doesn’t look the same for everyone - and it’s not always visible. Here's how the cycle often plays out:
Obsessions (Intrusive Thoughts or Urges):
Contamination fears:
“What if I touched something germy and brought illness home?”Violent intrusive thoughts:
“What if I suddenly lose control and hurt someone I care about?”Religious/guilt-based obsessions:
“What if I blasphemed or committed a sin without realizing it?”Sexual or identity-related thoughts:
“What if I’m sexually attracted to someone I shouldn’t be?”
(OCD UK highlights that the brain is powerful enough to trigger physical responses even to intrusive and distressing thoughts - especially in OCD themes around sexuality - making the fear feel intensely real and deeply confusing.)
These thoughts aren’t wishes. In fact, they’re the opposite - they go against a person’s values, which is what makes them so upsetting.
Compulsions (Actions or Mental Rituals to Neutralize the Thought):
Handwashing or cleaning: Over and over until it “feels right”.
Checking: Doors, gas knobs, appliances - again and again.
Mental rituals: Silently counting, praying, repeating phrases.
Avoidance: Skipping entire locations, people, or tasks out of fear of triggering obsessions.
While these behaviors may bring brief relief, they also reinforce the anxiety loop, making the OCD stronger over time.
Compulsions vs. Rituals: There’s a Subtle But Crucial Difference
The terms compulsions and rituals are often used interchangeably - and that makes sense, because in OCD, compulsions often take the form of ritualistic behavior. But as the International OCD Foundation clarifies, “not all repetitive behaviors or ‘rituals’ are compulsions”. Understanding the difference is key to identifying OCD and providing the right treatment.
A compulsion in OCD is an action (physical or mental) that’s performed to reduce anxiety, prevent harm, or neutralize a disturbing thought. These are typically unwanted, exhausting, and feel urgent. They’re driven by internal distress - not desire.
A ritual, however, while it may look similar on the outside (like repeated cleaning or checking), often comes with less internal resistance. In fact, rituals might be perceived by the person as the right or best way to do something. They are less “ego-dystonic”, meaning they don’t clash as painfully with the person’s own values or self-image.
For instance, a person might believe that a surface isn’t truly clean unless it’s scrubbed in a very particular sequence - and if the order is broken, they may feel compelled to start over. In such cases, the ritual might feel justified, even if it's time-consuming.
That said, not all compulsions are rituals - and not all rituals are compulsions. If someone showers excessively, but doesn’t follow a fixed sequence, it may not be ritualized. On the other hand, a ritual with a strict, repeated pattern - one that aims to reduce a fear or avert a specific outcome - could very well be a compulsion.
In essence:
Compulsions are driven by anxiety and performed to relieve it.
Rituals may be perceived as necessary or “correct” rather than distress-driven.
Many compulsions are ritualized, but not all rituals are compulsive.
The difference lies in the underlying drive - whether it’s anxiety and fear, or a rigid sense of “rightness”.
Inside the Mind: Key Characteristics of OCD
OCD isn’t just about being "extra neat" or "a bit anxious". At its core, it's a tangled loop of distress, doubt, and ritual - one that people don't choose, and often desperately want to break.
One key feature of OCD is that it’s ego-dystonic. That’s a fancy way of saying the thoughts and urges don’t align with who you are. They feel intrusive, distressing, and completely out of character. Imagine your mind sending you signals that go against your deepest values - that’s what ego-dystonic means. A person might have violent thoughts but feel horrified by them. Or they might be obsessing about harming someone they love, despite having no desire to do so.
This inner tug-of-war causes intense anxiety, which fuels the next phase: compulsions. These are actions - like checking, cleaning, or repeating - done to get relief. But it’s temporary. The anxiety creeps back in, and the cycle starts again.
Anxiety → Compulsion → Temporary relief → Anxiety again.
Interestingly, many adults with OCD know their behaviors don’t make logical sense, as the National Institute of Mental Health (NIMH) notes. Yet, they still feel trapped in performing them, because the fear of something terrible happening is overwhelming. It also mentions how children often lack the insight to recognize these rituals as irrational - they just know something bad might happen if they don’t comply.
This push-pull dynamic often leads to rumination - the mental replay button that never stops. It’s not just overthinking. Rumination is a vulnerability factor, a kind of cognitive trap that keeps feeding the OCD cycle. People get stuck analyzing their thoughts or actions endlessly, searching for certainty - and never finding it.
OCD isn't just a quirk. It's a deeply distressing condition where your own mind becomes the source of fear - and your actions, a desperate attempt to feel safe.
Symptoms of OCD: When Thoughts Take the Driver’s Seat
Everyone gets weird thoughts sometimes. But for someone with OCD, these thoughts don’t just pass through - they take the wheel, grip tight, and refuse to let go.
Obsessions are the starting point. These are not your everyday worries - they’re intrusive, persistent, and disturbing. They're not wanted, and they don’t feel good. The distress they cause can disrupt everything - sleep, work, relationships.
Some common obsessive themes include:
Fear of harm or causing harm, even accidentally
Fear of contamination or illness - germs, dirt, bodily fluids
Intrusive taboo thoughts - involving violence, sex, or religion
Fear of losing control - like shouting something offensive or doing something impulsive
A need for things to feel 'just right' or symmetrical
Then come the compulsions - the brain's attempt to neutralize those distressing thoughts:
Excessive cleaning/washing until skin is raw
Checking - doors, locks, stoves - again and again
Counting, tapping, or repeating specific actions a certain number of times
Arranging things until they’re “perfect”
Seeking constant reassurance, from loved ones or even Google
It's not the presence of these thoughts alone that defines OCD, but the distress and disruption they cause. If the thoughts or behaviors are affecting your quality of life, it’s more than a personality quirk - it’s a mental health condition.
And you’re not alone. OCD is treatable, and help is out there.
Decoding OCD: A Deep Dive into Common Subtypes
OCD is a shapeshifter - it doesn’t always look the same for everyone. While the underlying mechanism is the same (obsession + compulsion), the themes and triggers can differ wildly. Let’s explore the most common OCD subtypes:
1. Contamination OCD
The classic germ-fear. But it’s more than just being tidy - it’s a paralyzing fear of dirt, disease, or even emotional “contamination”. Some fear that touching certain people or objects might make them morally impure or absorb unwanted traits.
2. Harm OCD
Terrified of hurting someone - not because you want to, but because you’re scared you might. These thoughts are ego-dystonic, meaning they feel completely wrong. Still, the fear persists: “What if I snap?”
3. Sexual/Identity OCD (HOCD, POCD, ROCD)
These involve intrusive thoughts about sexuality, children, or relationships that clash painfully with the person's identity or values. More on this in the next section.
4. Religious/Moral OCD (Scrupulosity)
A consuming need to be morally or spiritually “pure”. People may pray repeatedly, seek forgiveness obsessively, or worry they’ve committed blasphemy.
5. Perfectionism OCD
Not just “wanting things neat” - this subtype drives people to endlessly redo tasks until they’re “just right,” often at the cost of time, relationships, and peace.
6. Existential OCD
Imagine your brain stuck on questions like “Why are we here?” or “What if none of this is real?” - not for curiosity, but from crippling anxiety. These philosophical spirals are endless and distressing, often leading to a deep sense of disconnection or dread.
7. Relationship OCD (ROCD)
People with ROCD obsess over whether their partner is "the one," if they feel enough love, or if a past relationship was better. They may check their feelings repeatedly, compare partners, or seek reassurance - all while feeling more confused and isolated.
8. Postpartum OCD
Unlike typical OCD, this form can emerge suddenly after childbirth, with terrifying thoughts of harming the baby or being a bad parent. It's not a sign of intent - it's a mental health condition, and treatable.
9. Symmetry and Order OCD
A powerful need for symmetry or things to be “just so”. People may spend hours arranging objects, redoing tasks, or feeling intense discomfort if something is out of place.
OCD can wear many masks - but no matter the subtype, you’re not alone, and your experience is valid.
HOCD, POCD, ROCD & OCD Spikes: The OCD Experience No One Talks About
These lesser-known OCD subtypes often come with deep shame, misunderstanding, and silence. But naming them is the first step to healing.
HOCD (Homosexual OCD or Sexual Orientation OCD)
This involves obsessive fears of being gay when you're straight - or vice versa. It's not about homophobia or confusion, but a relentless need for certainty. Every gesture, thought, or glance can feel like a sign - triggering panic. People may compulsively check their arousal, avoid same-sex individuals, or replay interactions mentally.
POCD (Pedophilia OCD)
One of the most distressing forms. People with POCD experience unwanted, intrusive thoughts about children - not because they desire them, but because they are terrified by them. These thoughts cause overwhelming guilt and shame, leading to compulsive behaviors like avoiding children, seeking reassurance, or checking their own feelings repeatedly.
ROCD (Relationship OCD)
Obsessions about romantic partners. “Do I really love them?” “What if they’re not right for me?” “What if I’m settling?” These aren’t just cold feet - they’re obsessive doubts, often followed by compulsions like comparing, analyzing, visualizing happy scenarios, or asking for constant validation.
OCD Spikes
As described by OCD UK, “spikes” generally refer to sudden, intense waves of distress triggered by an obsession. It’s like a mental ambush - out of nowhere, a thought grabs you, and the anxiety skyrockets. The spike includes the trigger, the obsession itself, and the distress that follows.
These spikes can feel like emotional whiplash. One moment you're fine, the next you’re overwhelmed, desperate for reassurance, and stuck in the OCD cycle again.
Each of these subtypes reflects the same underlying problem: intrusive thoughts + anxiety + compulsions. But because these themes are so misunderstood, many suffer in silence.
You are not your thoughts. OCD is lying to you - but support, therapy, and compassion can help you take your mind back.
“Obsessed” vs OCD: It’s Not What You Think
We’ve all heard phrases like “I’m so OCD about my desk!” or “She’s obsessed with that show!” - but there’s a world of difference between being passionate or particular and actually living with Obsessive-Compulsive Disorder (OCD).
OCD is not about enjoying routines, being tidy, or liking things a certain way. It's about intrusive, unwanted thoughts (obsessions) that trigger intense anxiety, and repetitive actions (compulsions) meant to neutralize that anxiety. These compulsions don’t bring satisfaction - only temporary relief, if any.
Think of it this way: passion drives you forward, OCD holds you hostage.
Let’s bust another myth while we’re at it:
OCD ≠ OCPD (Obsessive-Compulsive Personality Disorder).
As Rizvi A. and Torrico TJ explain in their book Obsessive-Compulsive Personality Disorder, OCD is defined by ego-dystonic experiences - people don’t want these thoughts or behaviors. They're distressing and feel alien. In contrast, OCPD traits are ego-syntonic - a person sees their need for control, order, and perfectionism as right, even if it creates friction with others.
So the next time someone says they’re “so OCD” because they like a neat planner or a spotless kitchen, it’s worth remembering: OCD isn’t about preference. It’s about persistent mental torment that most people would do anything to silence.
What Causes OCD? The Puzzle Pieces Behind the Disorder
OCD doesn’t have a single cause - it’s more like a puzzle made up of biology, life experiences, and even ancient bacteria.
Genetic Roots: Research shows that OCD often runs in families. Twin and family studies suggest that certain forms of OCD have a heritable component, meaning if a close relative has it, the risk increases.
Brain Chemistry & Structure: Some theories point to abnormalities in serotonin levels - a brain chemical involved in mood and behavior regulation. While it’s unclear whether this imbalance causes OCD or is an effect of it, it's a key area of focus in treatment.
Trauma and Stress: A history of trauma or intense stress can trigger or worsen OCD symptoms. The brain sometimes responds to trauma by trying to create “safety” through compulsive rituals or thoughts.
PANDAS: When Strep Affects the Mind
In children, a rapid onset of OCD symptoms can be linked to PANDAS (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections). Imagine waking up one day and your child is suddenly performing compulsive rituals, battling tics, or panicking about being apart from you.
Here’s why: Strep bacteria are sneaky. Through a process called molecular mimicry, they disguise themselves to look like healthy brain tissue. But once the immune system fights back, it may accidentally attack parts of the brain too - particularly those linked to behavior and emotion.
While PANDAS is still under investigation, its dramatic onset and symptoms are a reminder that OCD can be more than just psychological - it can be immunological.
Who’s at Risk? Understanding OCD’s Contributing Factors
OCD doesn’t discriminate - it affects people across all ages, genders, and cultures. But some factors can increase your likelihood of developing it:
Family History: If a parent, sibling, or close relative has OCD or an anxiety disorder, your risk goes up. Genetics play a key role, even if they’re not the full story.
Childhood Trauma: Experiencing neglect; emotional, physical, or sexual abuse - especially during formative years - can be a major trigger. The brain may learn to associate certain thoughts or actions with protection or safety.
Major Life Stressors: Moving, divorce, losing a loved one, or starting a new job or school - these stress points can all provoke OCD symptoms, particularly if they come on suddenly or are difficult to process emotionally.
Other Mental Health Conditions: OCD often coexists with anxiety disorders, depression, and sometimes ADHD or tic disorders. It’s not rare for individuals to navigate multiple mental health conditions at once.
Think of these factors as fuel - they don’t guarantee the fire of OCD will start, but under the right conditions, they can fan the flames.
Related Disorders: When It’s Not Just OCD
OCD often overlaps with or gets confused with other conditions that involve compulsions, obsessions, or body-focused repetitive behaviors. Understanding the differences can lead to better care.
Body Dysmorphic Disorder (BDD)
Both BDD and OCD involve repetitive checking. But in BDD, the obsession centers exclusively on appearance. Individuals may fixate on perceived flaws, often seeking cosmetic procedures. People with OCD don’t usually have thoughts or rituals linked to their looks.
Trichotillomania (Hair Pulling)
This isn’t about “playing with your hair” - it’s a clinical disorder. To be diagnosed, the person must have repeated hair pulling that leads to noticeable hair loss, feel unable to stop, and experience significant distress or disruption. The APA clarifies that it must not be due to a medical or another mental condition.
Excoriation Disorder (Skin Picking)
Similar to trichotillomania, but the focus is on skin. People pick at real or perceived blemishes, often to the point of injury or infection. It’s not a simple habit - it’s compulsive and emotionally distressing.
Tic Disorders & GAD
Tics (sudden, repetitive movements or sounds) and Generalized Anxiety Disorder (GAD) may co-occur with OCD. While GAD involves persistent worrying, OCD is more specific - compulsions arise from intrusive thoughts that demand neutralization.
Each of these conditions is unique, but they share a thread: repetitive thoughts or actions that interfere with daily life. Understanding their nuances matters.
Postpartum OCD: The Silent Struggle After Birth
We often hear about Postpartum Depression, but what if your mind suddenly floods with terrifying thoughts of harming your baby - and you’re horrified by them?
This is Postpartum OCD, and it’s more common than most people think. It typically emerges shortly after childbirth and involves disturbing, unwanted thoughts (obsessions) - often about harming the baby - even though the parent would never actually do so. To reduce the anxiety caused by these thoughts, they may develop compulsions, like checking locks, avoiding the baby, or cleaning excessively.
These thoughts are not psychotic hallucinations. People with Postpartum OCD know the thoughts are irrational and upsetting. That’s what makes it so distressing - they feel out of control, but they’re fully aware.
What’s more, fathers can experience it too, as highlighted by the Postpartum Depression Org. Dads may also have intrusive thoughts or compulsions related to their child’s safety and their own parenting.
This condition is often mistaken for Postpartum Depression or Psychosis, but it’s a different experience altogether. And because of the shame attached, many parents suffer in silence.
Postpartum OCD needs specialized, compassionate care - not judgment. With therapy, particularly CBT and Exposure and Response Prevention (ERP), many parents recover and bond healthily with their baby again.
OCD in Children: When OCD Comes Out of the Blue
We’ve touched on this earlier while discussing PANDAS - a rare but eye-opening condition where a simple strep throat could flip a child’s world upside down. To recap:
PANDAS stands for Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections. It’s when OCD or tics suddenly emerge or worsen dramatically after a strep infection, often “overnight and out of the blue”. These children may develop motor or vocal tics, intense obsessions or compulsions, anxiety, separation fears, and even mood swings.
This isn’t your usual gradual onset of OCD. It’s rapid, jarring, and deeply distressing - both for the child and their caregivers. Scientists believe this happens due to a case of molecular mimicry, where the immune system - in trying to fight the bacteria - mistakenly attacks parts of the child’s brain involved in behavior and emotion.
While research is still evolving, PANDAS highlights how OCD can manifest early and in deeply biological ways, sometimes without any psychological trigger at all.
Diagnosing OCD: What the DSM-5 Really Says
OCD isn’t diagnosed on a whim - it’s defined with precision. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5), issued by the American Psychiatric Association, outlines clear-cut criteria to ensure OCD is properly identified.
According to the DSM-5, OCD consists of:
Obsessions, which are:
Intrusive, unwanted thoughts, urges, or images that cause intense anxiety or distress.
The individual attempts to suppress or neutralize them (often by performing a compulsion).
Compulsions, which are:
Repetitive behaviors or mental rituals (like handwashing, counting, praying) that the person feels driven to perform to reduce their anxiety or prevent a feared event.
But these actions are not realistically connected to the feared event, or are clearly excessive.
Plus, to qualify as OCD:
These obsessions and/or compulsions must be time-consuming (typically more than 1 hour per day),
Or cause significant distress or impair the person’s social, occupational, or daily functioning.
This diagnostic clarity is critical. It draws the line between occasional worry or routine and a disorder that hijacks time, peace, and well-being.
Other Shades of OCD: When It Gets Complicated
OCD isn’t a static condition - it can shift, morph, and co-exist with other psychological states. Some features are less talked about, but they matter deeply.
🌩 Anxious Distress
It’s common, almost expected. But sometimes, this anxiety becomes chronic, intense, and deeply debilitating - fueling the obsessive-compulsive loop further.
🌑 Melancholy & Depression
Some individuals with OCD sink into melancholic depression, especially when compulsions feel inescapable or when obsessions attack core aspects of their identity.
🌀 Psychosis (Rare, But Real)
While rare, in some severe cases, OCD can be a precursor to psychotic symptoms. Obsessions might blend into delusional thinking, or the compulsions may take on bizarre, ritualistic qualities disconnected from logic or reality.
🌪 Mixed States: Mania + OCD
Occasionally, OCD overlaps with mania, especially in people with bipolar tendencies. This can result in erratic energy, hyper-focused compulsions, and intensified intrusive thoughts — making diagnosis and treatment more complex.
🔄 Rapid Cycling
Some experience obsessions and compulsions that evolve quickly, even within a single day or week - a storm of mental loops that rarely settles.
🤰 Hormones, Pregnancy & Seasonal Shifts
Pregnancy and hormonal changes can worsen OCD symptoms. Some individuals also report that OCD intensity varies with seasons, often flaring up during winter months.
Recognizing these layers helps demystify the rich and often challenging reality of living with OCD - a disorder that’s never one-size-fits-all.
Current Treatments for OCD
Here’s the hopeful part - OCD is treatable. The path isn’t always easy, but with the right combination of therapy, tools, and support, recovery is within reach.
🧠 Therapy is First-Line - and for Good Reason
Cognitive Behavioral Therapy (CBT): Rewiring the Thought Loop
Insert this YouTube Video: CBT for obsessive compulsive disorder (OCD)
CBT is a structured, skills-based approach that helps individuals recognize the patterns between obsessive thoughts, emotional distress, and compulsive behaviors. The goal? To interrupt the loop, reframe thoughts, and regain control.
CBT doesn’t ask people to ignore their distress. Instead, it equips them with tools to challenge distorted thinking, reduce avoidance, and respond to obsessions more rationally.
📊 In a controlled study of 40 individuals with OCD, 82.5% reported significant symptom improvement following CBT. Even more compelling: 57.5% achieved clinically significant results - a milestone that translates to real-life relief, not just better scores on paper.
CBT is especially effective when combined with ERP (Exposure and Response Prevention), which is often embedded within the CBT framework for OCD.
Exposure and Response Prevention (ERP): The Gold Standard
Insert this YouTube Video: ERP Therapy for OCD | A Complete Guide | #PaigePradko, #OCDwithPaige, #OCD
ERP is widely regarded as the gold standard for OCD treatment - and with good reason. It involves intentionally confronting feared thoughts or situations (exposure), while deliberately resisting the urge to perform compulsions (response prevention).
This process gradually helps the brain unlearn the association between obsessive thoughts and immediate danger.
But it’s not easy. The International OCD Foundation tells you to expect this when ERP is done properly:
You’ll initially feel more anxious, not less. Obsessions may spike. That’s a normal and expected part of the process.
You learn that these thoughts - while distressing - are not dangerous. The fear loses its grip.
Anxiety naturally fades over time as your brain habituates to the discomfort.
You reclaim confidence, learning that uncertainty can be tolerated, and that avoidance is not the only way to feel safe.
ERP changes how your brain processes fear and discomfort. It’s not about forcing yourself to be “okay” - it’s about learning to live without fear controlling your actions.
Acceptance and Commitment Therapy (ACT): Living with Meaning, Not Fear
Insert this YouTube Video: The OCD Mind and Uncertainty | ACT
ACT takes a slightly different approach. Rather than trying to eliminate intrusive thoughts, ACT helps individuals accept them as passing mental events, without judgment or over-identification.
The goal of ACT isn’t to suppress thoughts - but to shift your relationship to them. You learn to:
Allow distress to exist without acting on it.
Stop avoiding situations based on fear.
Live in alignment with your values, even if OCD symptoms persist in the background.
In a study by Soondrum, Tamini et al., ACT was found to significantly reduce OCD severity, with a large effect size on the YBOCS (Yale-Brown Obsessive Compulsive Scale) - a widely used clinical measure.
ACT can be especially effective for individuals with chronic OCD, those who’ve hit a wall with traditional methods, or anyone looking to improve overall quality of life alongside symptom relief.
🖥️ Online OCD Therapy with Elfina Therapists
You don’t need to sit in traffic or navigate waiting rooms to get life-changing OCD support. At Elfina, we bring evidence-based therapy directly to you - wherever you are.
Whether it’s ERP, CBT, or ACT, our expert clinicians are trained in the gold-standard treatments for OCD and tailor each session to your unique experience. Our therapists understand that OCD isn’t “one size fits all,” and neither is recovery. That’s why:
We match you with therapists who specialize in OCD - not generalists.
You’ll receive structured, science-backed care designed for your specific obsessions and compulsions.
We offer a private, judgment-free space where you can work through fears safely and openly.
Sessions are available online and on your schedule - because healing should work with your life, not against it.
With Elfina, therapy isn’t just convenient. It’s effective, accessible, and deeply personal.
💊 Medication
Often used alongside therapy, the NHS recommends SSRIs (Selective Serotonin Reuptake Inhibitors) as the first-line medication. They boost serotonin, a brain chemical involved in mood and anxiety.
It may take up to 12 weeks to see results, and like any medication, SSRIs can have side effects:
Feeling agitated or anxious
Nausea, dizziness, or headaches
Sleep issues or sexual side effects
🏡 Home Remedies & Self-Care That Actually Help
Journal your thoughts instead of acting on them. Let them exist on the page - not in your behavior.
Practice mindfulness - not just meditation, but grounding exercises, mindful walks, or sensory resets.
Reduce caffeine and stress - both amplify anxiety and compulsive urges.
Stick to routines and sleep schedules - stability helps the mind stay regulated.
💛 How to Support Someone with OCD
Watching someone you love struggle with OCD can feel overwhelming - but your support matters more than you know. Here’s how to show up with compassion and make a real difference.
1. Don’t Dismiss or Minimize Their Distress
OCD isn’t about “being dramatic” or “overthinking”. To the person experiencing it, their fears and compulsions feel very real. Avoid comments like “just relax” or “stop thinking about it” - these can unintentionally invalidate their experience.
Instead: Try, “That sounds really tough. I’m here for you.”
2. Don’t Enable – But Be Gentle
You may be tempted to help them avoid triggers or participate in rituals to reduce their anxiety - but this only reinforces OCD's grip.
Be supportive without feeding the cycle. If you're unsure how to navigate this, involve a therapist early on for guidance.
Try saying:
"I know this feels urgent right now. Would you like to try something we discussed in therapy instead?"
3. Be Patient with Their Recovery
OCD recovery isn’t linear. There will be progress, setbacks, victories, and relapses. Avoid rushing their healing or expecting “quick fixes”. Your consistent, non-judgmental presence is one of the best things you can offer.
4. Educate Yourself
Learn about OCD - not just the symptoms, but the science behind them. The more you understand, the more helpful and empathetic you can be.
Support doesn’t mean solving the problem. It means standing beside someone while they learn to solve it themselves.
🚫 What’s Not OCD
Let’s clear something up: OCD is not a personality trait, a joke, or a punchline. Misusing the term can minimize the lived experiences of people who struggle with it every day. Here’s what OCD isn’t:
❌ Liking Things Clean or Organized
Neatness or attention to detail isn’t the same as OCD.
A preference for clean spaces doesn’t involve distressing, repetitive thoughts or compulsive behaviors performed to reduce anxiety.
“I’m so OCD about my desk” is not only inaccurate - it’s dismissive.
❌ Having Routines or Quirks
Routines can be comforting. OCD compulsions, on the other hand, feel urgent and intrusive. They’re performed not out of habit, but out of a perceived need to prevent harm, discomfort, or catastrophe.
❌ A Quirky Personality Trait
OCD is a clinical diagnosis - a serious mental health condition. It involves real suffering and often interferes with relationships, careers, and daily functioning. Using "OCD" as slang only fuels misunderstanding and stigma.
Understanding what OCD isn’t helps us take what it is more seriously - and support those who need help more effectively.
🌐 Getting Diagnosed & Treated Online
Worried you might have OCD? Or maybe you’ve already been struggling in silence for years. Help is closer than you think.
At Elfina, we make expert OCD care available right from your home.
Here’s what makes Elfina’s online therapy stand out:
✔️ Evidence-Based Treatment
We use CBT, ERP, and ACT - the most effective, science-backed therapies for OCD. No fluff. Just proven methods that help you feel better.
🧠 Experienced OCD Specialists
Over 80% of our therapists have more than 5 years of experience treating complex conditions like OCD, anxiety, mood disorders, and burnout. You’re not getting a generalist - you’re getting a match who understands your specific needs.
⏱️ Flexible, Judgment-Free Support
You pick the time and place. Sessions are conducted online, so you can open up from wherever you feel safest.
🔒 Complete Privacy
Therapy should be safe in every sense. We offer a confidential, non-judgmental space to explore what’s going on inside your mind - and begin to untangle it with guidance and care.
🎯 94% of our clients find the right therapist on their first match - saving time, emotional energy, and unnecessary trial and error.
Conclusion: Your Path to Relief Starts Here
OCD can be isolating, overwhelming, and exhausting - but you don’t have to face it alone.
With the right tools, the right support, and the right therapy, relief is possible.
At Elfina, we understand OCD from both a clinical and human lens. Whether you’re just starting to question your symptoms or deep into your recovery journey, we’re here with:
Deep expertise in OCD and related disorders
Therapists who listen without judgment
Personalized treatment plans grounded in evidence
An online platform designed for comfort, flexibility, and long-term support
Your story with OCD doesn’t end at fear or frustration.
It can end at freedom.
Start your journey today - connect with an Elfina therapist who gets it.
Because better days aren’t just possible. With Elfina, they’re within reach. 💙
Other blogs

Frequently Asked Questions
What types of therapy do you offer?
Can I meet my therapist in-person?
How do you match me with a therapist?
How much does therapy cost?
Do you offer free trials?
Finding The Right Fit, Made Easy





© Mindaro Health Technologies. All rights reserved
© Mindaro Health Technologies. All rights reserved
Finding the right fit, made easy.
FAQs
What types of therapy do you offer?
Can I meet my therapist in-person?
How do you match me with a therapist?
How much does therapy cost?
Do you offer free trials?