
It’s Not Always About the Food: Understanding, Treating & Healing from Eating Disorders
|
13
min read
|
Tanvi

It’s Not Always About the Food
A college student becomes obsessed with “clean eating”. No sugar, no oil, no dinners out. She’s praised for her discipline - until she stops showing up altogether.
A teenage boy spends hours at the gym and is flooded with likes on his shirtless photos. No one sees the binge–guilt–starve cycle he’s stuck in.
These aren’t stories of vanity.
They’re stories of control, shame, and a quiet desperation to feel okay.
Myth: You can “see” an eating disorder
Reality: Many eating disorders don’t look like what we expect. They don’t always involve extreme thinness.
They can hide behind:
“Wellness” routines
Intermittent fasting
Gym obsession
“Good discipline”
In India especially, we mistake early signs for self-control. We compliment the person who skips meals, praises khichdi and lemon water, or fasts even when exhausted.
But suffering doesn’t always look sick.
What the data says
A 2018 study in Mysore found that over 26% of students showed signs of disordered eating.
In Bangalore, 66% of psychiatrists had seen at least one eating disorder case in the past year.
Cultural factors - like peer pressure, appearance-based marriage markets, and weight-related comments - often play a hidden but powerful role.
Despite rising cases, India still lacks comprehensive national data on eating disorders - a silence that’s part of the problem.
What Are Eating Disorders?
Eating disorders are not diets gone wrong.
They are serious, diagnosable mental health conditions that impact how people eat, think, feel, and function.
Clinical definition (DSM-5-TR):
“A persistent disturbance of eating or eating-related behaviour that results in the altered consumption or absorption of food and that significantly impairs physical health or psychosocial functioning.”
This could mean:
Restricting food out of fear
Binge eating until numb
Obsessively “eating clean”
Feeling deep guilt after every meal
It’s not a phase or a choice
It’s not about vanity.
It’s about coping - with trauma, low self-worth, control issues, or anxiety.
And it can affect anyone - regardless of gender, age, caste, body size, or income.
Still, in India, many go undiagnosed - either due to stigma or lack of awareness, even among professionals.
Types of Eating Disorders
Eating disorders are not just about food - they are about pain, identity, control, and how that pain gets expressed through eating patterns, rituals, or avoidance. These conditions can look vastly different across people and cultures. One person may be severely restricting calories; another might binge in secret and live in shame; a third may obsess over "clean eating" while slowly disappearing into anxiety.
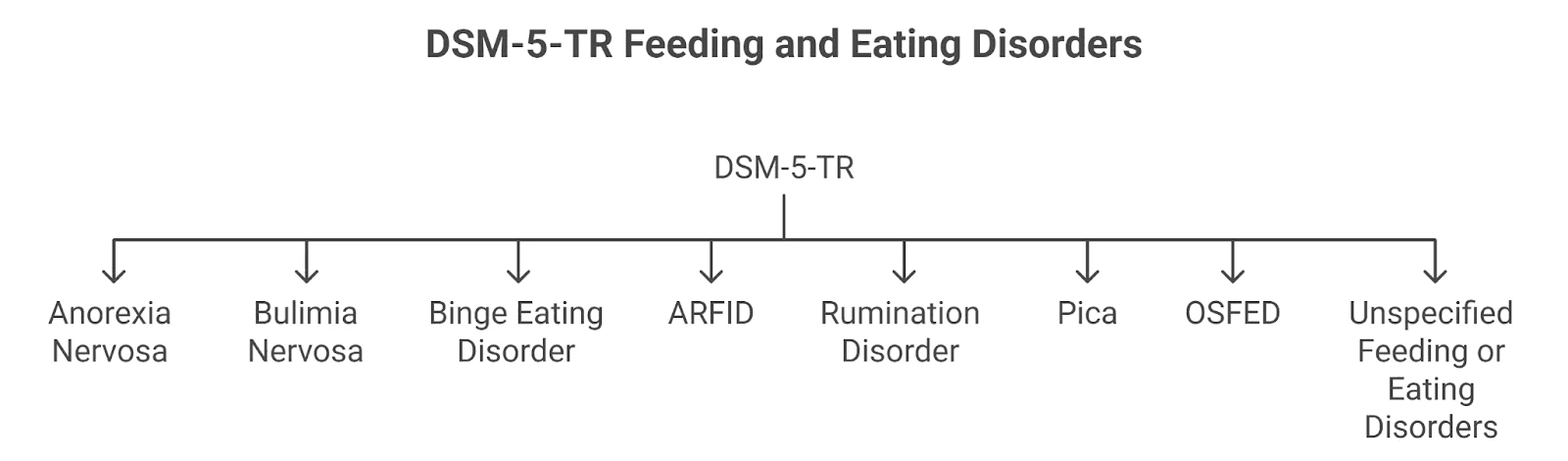
The DSM-5-TR (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision) currently outlines eight clinically recognised feeding and eating disorders, each with distinct diagnostic criteria and severity levels. These include Anorexia Nervosa, Bulimia Nervosa, Binge Eating Disorder, ARFID, Rumination Disorder, Pica, Other Specified Feeding or Eating Disorders (OSFED), and Unspecified Feeding or Eating Disorders.
In this section, we’ll explore each of these diagnoses using the DSM-5’s official diagnostic criteria - alongside lived realities, emerging research, and cultural factors that shape how eating disorders show up, especially in Indian contexts.
Anorexia Nervosa
"I’m not thin enough. I’m never thin enough."
Anorexia isn’t about vanity - it’s often about control in a world that feels chaotic.
People with anorexia engage in extreme restriction, fuelled by a distorted body image and an intense fear of gaining weight.
Diagnostic Criteria (DSM-5):
A. Restriction of energy intake leading to significantly low body weight (relative to age, sex, developmental stage, and health).
B. Intense fear of gaining weight or persistent behaviour that prevents weight gain - even when underweight.
C. Distorted body image or an inability to recognise the seriousness of current low weight.
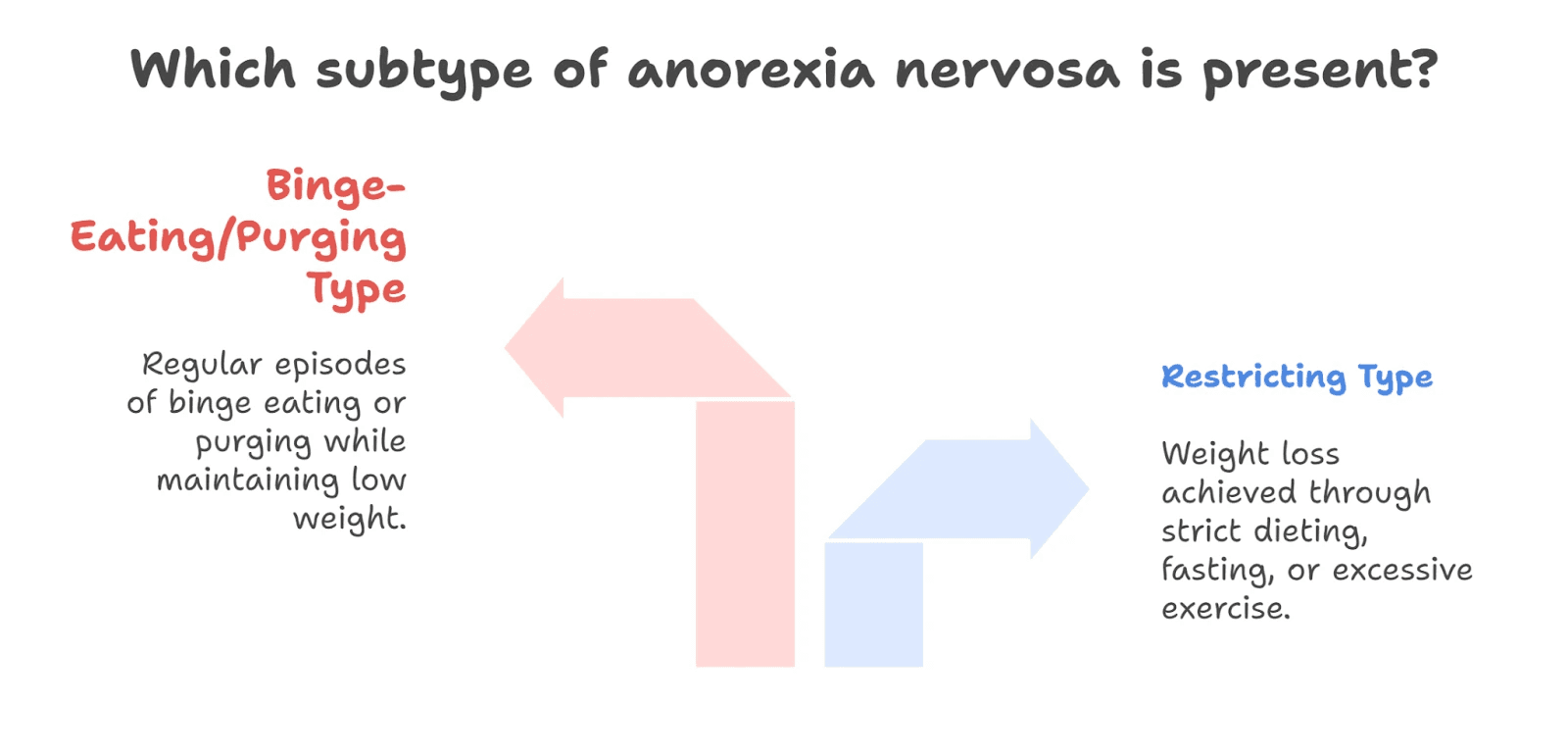
Subtypes (as per Eating Disorder Resources):
Restricting Type: Weight loss achieved through strict dieting, fasting, or excessive exercise.
Binge-Eating/Purging Type: Regular episodes of binge eating or purging (vomiting, laxatives) while still maintaining a significantly low weight.
Important: A person does not need to be underweight to be diagnosed with anorexia. Larger-bodied individuals can still meet all other criteria - but often go undiagnosed due to cultural weight stigma.
Remission Specifiers:
Partial Remission: Weight has returned to a healthier level, but fear of weight gain or body image issues remain.
Full Remission: No criteria have been met for a sustained period.
Levels of Severity (as per AAFP):
Severity | BMI Range |
Mild | ≥ 17 kg/m² |
Moderate | 16–16.99 kg/m² |
Severe | 15–15.99 kg/m² |
Extreme | < 15 kg/m² |
Diagnostic Crossovers:
A landmark study found that most women with anorexia transitioned between subtypes over time - and some shifted to bulimia before often reverting back to anorexia. This tells us how fluid and complex eating disorders can be.
Pop Culture Reference:
Nina in Black Swan - driven by perfection, fear, and control - reflects the haunting emotional world of someone with anorexia.
Bulimia Nervosa
“I binge until I feel numb - then I punish myself.”
Bulimia often hides behind smiling faces and “normal” bodies.
It involves cycles of binge eating, followed by compensatory behaviors like vomiting, excessive exercise, or starvation.
Diagnostic Criteria (DSM-5):
A. Recurrent episodes of binge eating. Each episode involves:
Eating an amount of food larger than typical in a short time (e.g., 2 hours)
Feeling out of control during the episode
B. Recurrent inappropriate compensatory behaviors to prevent weight gain - such as vomiting, laxatives, fasting, or over-exercising.
C. These behaviors occur at least once a week for 3 months.
D. Self-worth is disproportionately influenced by body shape and weight.
E. The disturbance doesn’t occur exclusively during episodes of anorexia nervosa.
Levels of Severity (as per AAFP):
Severity | Episodes of compensatory behavior per week |
Mild | 1–3 episodes |
Moderate | 4–7 episodes |
Severe | 8–13 episodes |
Extreme | 14+ episodes |
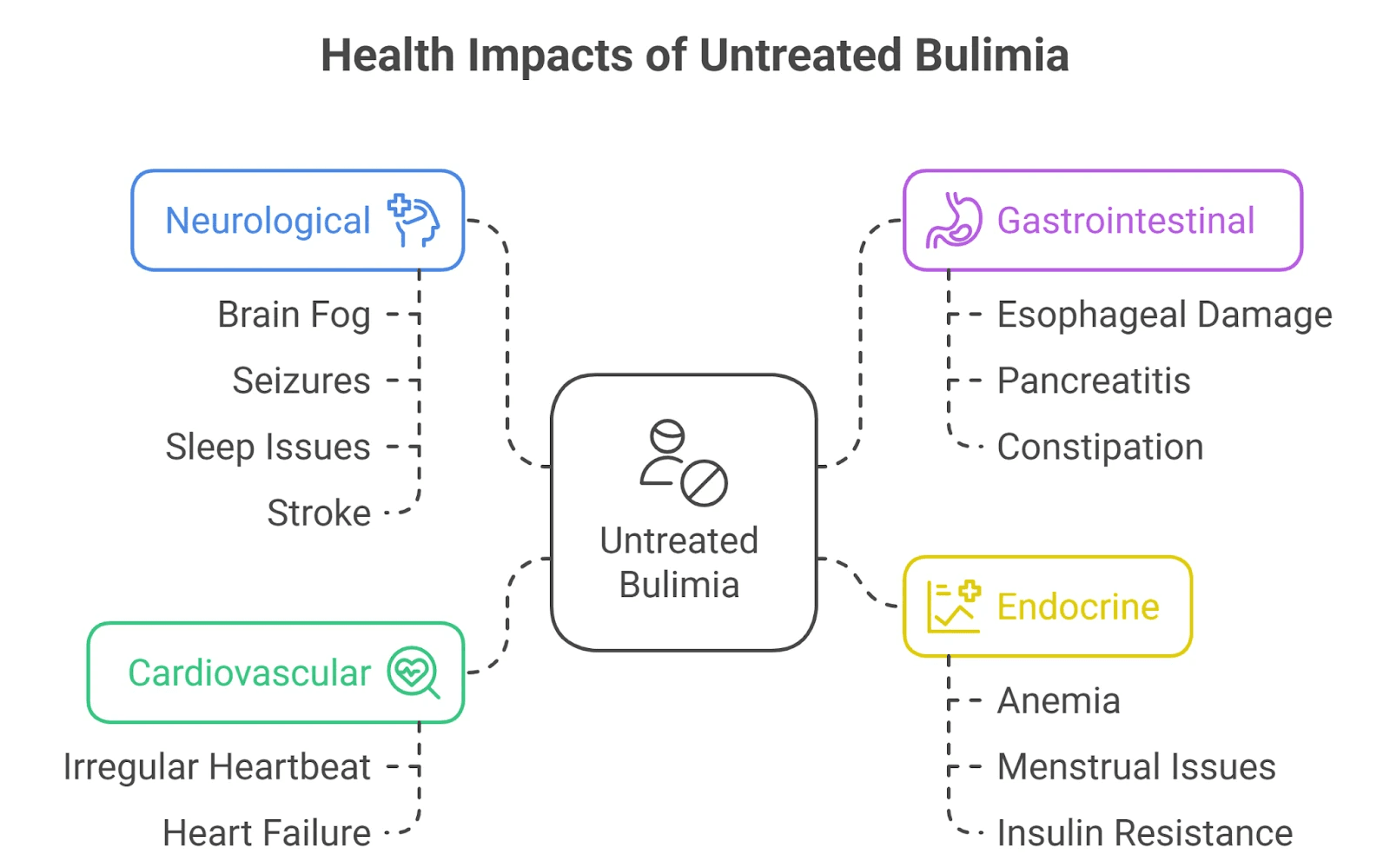
Health Consequences (if untreated):
According to Psych Central, untreated bulimia can affect nearly every system:
Cardiovascular: Irregular heartbeat, heart failure
Gastrointestinal: Esophageal damage, pancreatitis, constipation
Endocrine: Anemia, menstrual issues, insulin resistance
Neurological: Brain fog, seizures, sleep issues, stroke
When It Begins - and Who It Affects:
According to the Children’s Hospital of Philadelphia, bulimia most often begins in adolescence or early adulthood. It’s more common in girls than boys, but it can affect people of any gender.
Despite its often-invisible presentation, bulimia carries a high emotional and physical toll, and in some cases, a higher risk of suicide than anorexia nervosa due to intense depressive symptoms and self-loathing.
What Binges Look Like:
Binges often involve high-calorie foods people normally restrict - sweets, fried foods, bread. It’s not hunger; it’s emotional overwhelm, followed by purging to feel in control again.
Real-Life Reference:
Princess Diana openly shared her struggles with bulimia - breaking silence in a world that often rewards appearance and ignores inner pain.
Binge Eating Disorder (BED)
“Sometimes I eat until I feel sick - and then I cry in shame.”
Binge Eating Disorder (BED) is one of the most common but misunderstood eating disorders. Unlike bulimia, there are no compensatory behaviors like purging or over-exercising. And unlike anorexia, weight loss is not a defining feature. At its core, BED is about losing control around food, feeling immense guilt afterward, and falling into a cycle of emotional distress.
Many people with BED appear to function “normally” in daily life - going to work, raising families, meeting deadlines - while battling overwhelming episodes of binge eating in private. It's not simply “overeating” or “laziness”. It’s a mental health condition rooted in emotion regulation, trauma, and often years of dieting or shame.
DSM-5 Diagnostic Criteria for Binge Eating Disorder:
A. Recurrent episodes of binge eating. Each episode is defined by both:
Eating, in a short period (e.g., 2 hours), an amount of food significantly larger than most people would eat under similar circumstances.
A sense of lack of control during the episode.
B. Binge-eating episodes are associated with at least three of the following:
Eating much more rapidly than normal
Eating until uncomfortably full
Eating large amounts when not physically hungry
Eating alone due to embarrassment
Feeling disgusted, depressed, or very guilty afterward
C. Marked distress regarding binge eating.
D. The behavior occurs at least once a week for three months.
E. The binge eating is not associated with compensatory behaviors (i.e., not bulimia or anorexia).
Severity Levels (as per PsychDB):
Severity | Episodes of binge eating per week |
Mild | 1–3 episodes |
Moderate | 4–7 episodes |
Severe | 8–13 episodes |
Extreme | 14+ episodes |
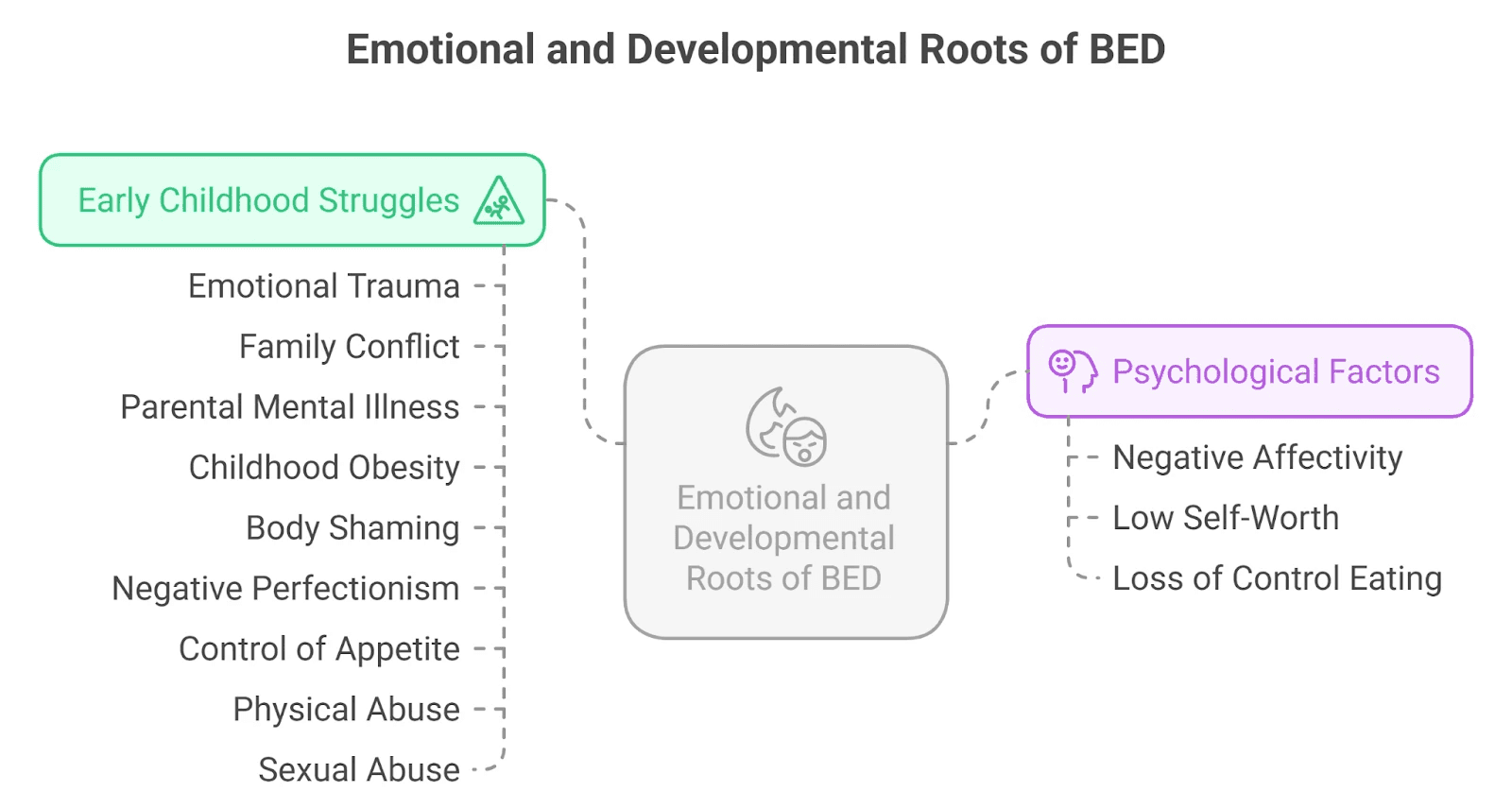
Emotional and Developmental Roots:
BED isn’t just about food - it’s about feelings. Many people report early childhood struggles, such as:
Emotional trauma, family conflict, or parental mental illness
Childhood obesity and body shaming
Negative perfectionism or feeling “never good enough”
A history of being told to “control” one’s appetite or weight
Physical or sexual abuse
Psychologically, negative affectivity, low self-worth, and a history of loss of control eating in childhood are common precursors.
In Remission:
Partial remission: Binge eating occurs less than once per week for a sustained period
Full remission: No binge episodes or distress for a sustained period
Avoidant/Restrictive Food Intake Disorder (ARFID)
“I’m not scared of gaining weight - I’m scared of eating at all.”
ARFID is a lesser-known but serious eating disorder that’s not driven by body image concerns. Instead, individuals with ARFID struggle with extreme food avoidance - often because of sensory aversions, lack of interest in food, or fear of choking, vomiting, or discomfort.
This condition is often mistaken for “just picky eating”, especially in children, but the consequences can be severe - from malnutrition and stunted growth to social isolation and emotional distress.
DSM-5 Diagnostic Criteria for ARFID:
A. An eating or feeding disturbance (e.g., apparent lack of interest in eating or food; avoidance based on sensory characteristics of food; fear of aversive consequences of eating) manifested by persistent failure to meet nutritional or energy needs, associated with one or more of the following:
Significant weight loss (or failure to gain weight or grow as expected)
Significant nutritional deficiency
Dependence on nutritional supplements or tube feeding
Marked interference with psychosocial functioning
B. The disturbance is not due to food unavailability or culturally sanctioned practices (e.g., religious fasting).
C. The eating disturbance is not due to body image issues - differentiating it from anorexia or bulimia.
D. If occurring alongside another medical or mental condition, the severity of eating disturbance must be clinically significant and beyond what’s typical for that condition.
What ARFID Can Look Like:
A child who refuses to eat anything but plain white rice or biscuits
A teen who fears vomiting after a past choking incident
An adult who lives on protein shakes due to strong taste or texture aversions
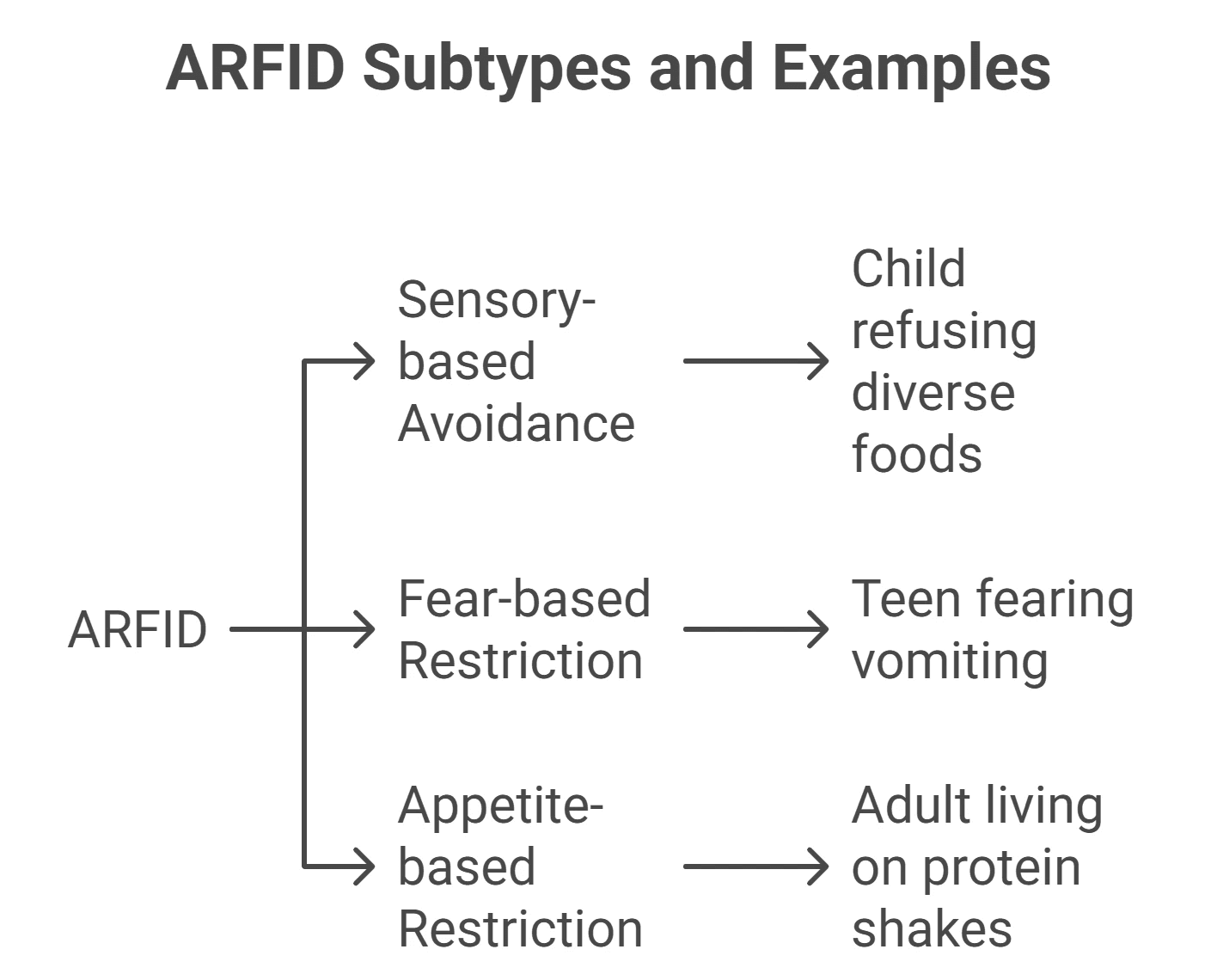
There are three common subtypes of ARFID:
Sensory-based avoidance (due to smell, texture, taste)
Fear-based restriction (fear of choking, vomiting, etc.)
Appetite-based restriction (very low hunger or interest in food)
Medical Consequences:
As per clinical literature, untreated ARFID can lead to:
Nutritional deficiencies (iron, calcium, vitamins)
Electrolyte imbalances
Bradycardia (slow heart rate), fainting
Gastrointestinal issues, bone loss
Amenorrhea (loss of menstruation in those assigned female at birth)
Important to Know:
ARFID is not “just a phase” or something people “grow out of”. Children who don’t outgrow early picky eating - or who experience trauma related to food - may develop ARFID, and the condition often continues into adolescence or adulthood if untreated.
Other Specified Feeding or Eating Disorders (OSFED)
“I’m not ‘sick enough’ to count - but I’m still suffering.”
Not every eating disorder fits into a neat clinical box. In real life, people often display serious, even dangerous, symptoms - but don’t meet the full criteria for anorexia, bulimia, or binge eating disorder. That’s where OSFED comes in.
OSFED stands for Other Specified Feeding or Eating Disorders, and it’s the most commonly diagnosed eating disorder in many countries, including India. Cultural masking - like calling disordered patterns “good discipline”, “fasting”, or “clean living” - can obscure how severe the struggle really is.
DSM-5 Definition:
OSFED is diagnosed when someone experiences clinically significant symptoms of a feeding or eating disorder, but the presentation doesn’t meet the full diagnostic criteria for other eating disorders.
Importantly, OSFED is not “less serious”. A meta-analysis found that adolescents with OSFED were just as likely to be hospitalized as those with anorexia nervosa.
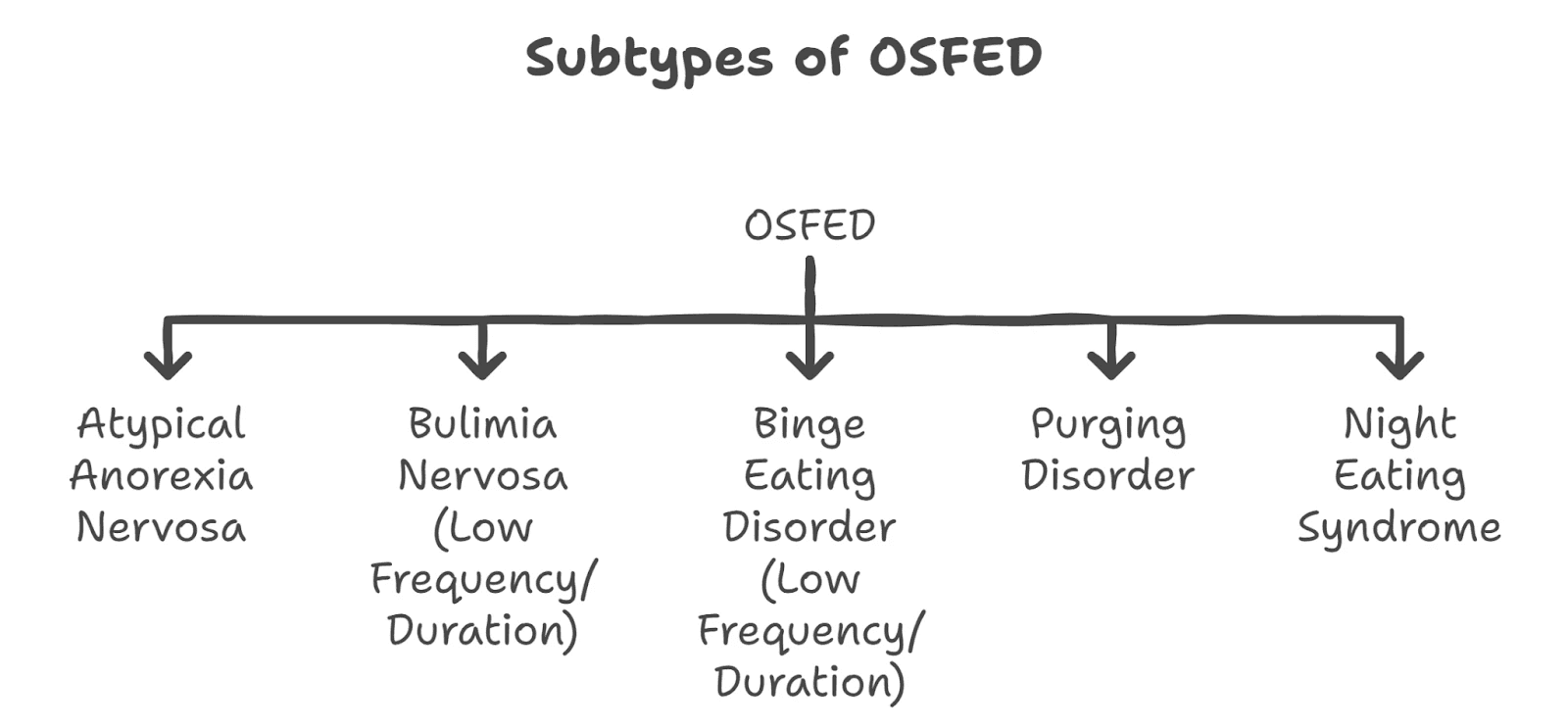
Subtypes of OSFED (DSM-5):
Atypical Anorexia Nervosa
All criteria for anorexia nervosa are met, except the person is not underweight. This is especially common in India, where people in higher-weight bodies may be overlooked or even encouraged to continue restrictive eating.Bulimia Nervosa (Low Frequency/Duration)
Meets all bulimia criteria, but bingeing and purging occur less than once a week or for less than 3 months.Binge Eating Disorder (Low Frequency/Duration)
Binge episodes happen less frequently or for a shorter period, but still cause significant distress.Purging Disorder
Regular purging (vomiting, laxatives, etc.) without bingeing.Night Eating Syndrome
Repeatedly eating after waking from sleep or consuming excessive food post-dinner, with full awareness. This causes significant distress and is not due to lifestyle, cultural norms, or other medical conditions.
Why It’s So Common in India:
Many people fast for religious or “discipline” reasons - masking harmful patterns
Weight stigma can lead people in larger bodies to go undiagnosed
Cultural silence around food, appearance, and distress makes it harder to name the issue
Individuals with OSFED may feel like they’re “not sick enough” to deserve help - but they are.
Rumination Disorder
“I keep regurgitating my food - I don’t know why, and I feel ashamed.”
Rumination Disorder may sound unusual, but it’s a real and serious condition - characterised by repeated regurgitation of food, which may be re-chewed, re-swallowed, or spit out. It’s not due to nausea or a medical problem like reflux. And while it’s more common in infants and people with developmental disabilities, it can occur in adults too.
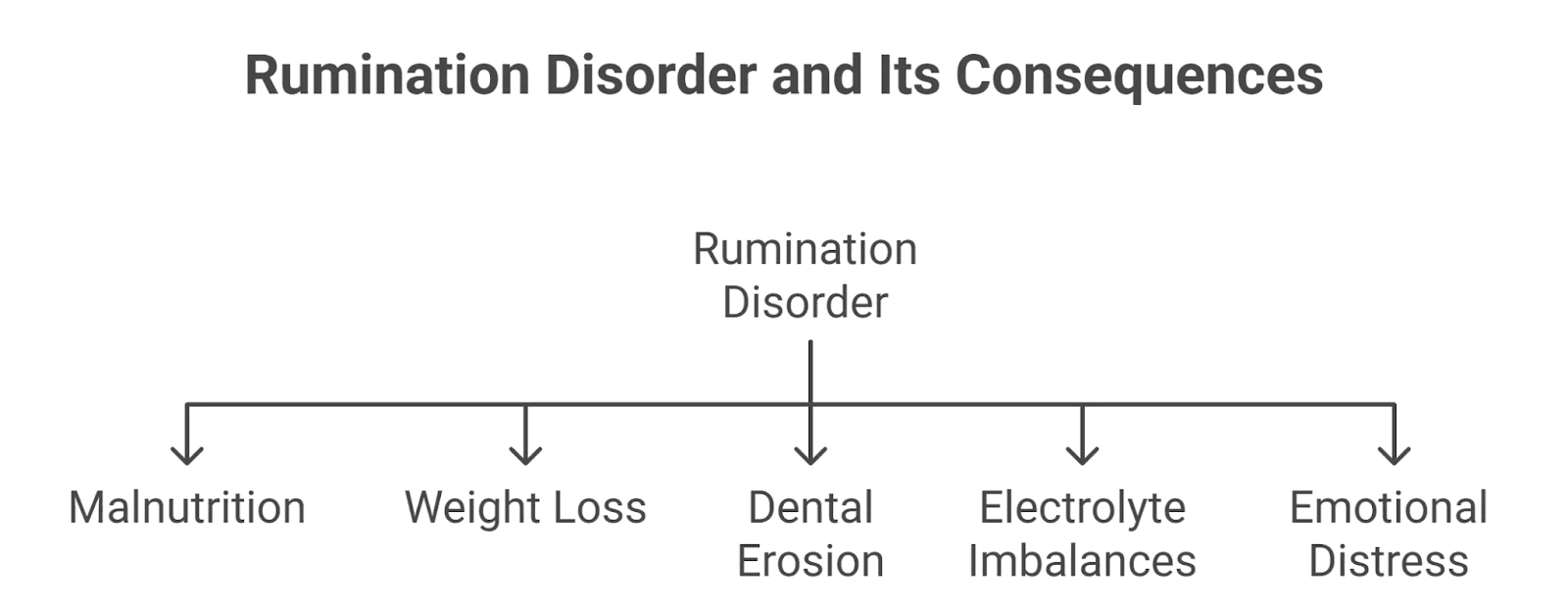
Often dismissed as “weird” or mistaken for a physical issue, Rumination Disorder can lead to malnutrition, weight loss, dental erosion, electrolyte imbalances, and emotional distress if left untreated.
DSM-5 Diagnostic Criteria:
A. Repeated regurgitation of food over a period of at least 1 month. This may include re-chewing, re-swallowing, or spitting the food out.
B. The behavior is not due to a medical condition like gastroesophageal reflux or pyloric stenosis.
C. The disturbance does not occur exclusively during anorexia, bulimia, BED, or ARFID.
D. If it occurs alongside a neurodevelopmental condition (e.g., intellectual disability), the behavior is severe enough to warrant clinical attention.
Why It’s Misunderstood:
People may hide it out of embarrassment
It can be misdiagnosed as reflux, nausea, or vomiting
In adults, especially, it's often ignored or wrongly classified
Important Clarification:
While Rumination Disorder is listed separately from OSFED in the DSM-5, some clinicians may include it under the OSFED umbrella in practical contexts - especially when the presentation doesn’t fully meet criteria or co-occurs with other disordered eating behaviors.
Unspecified Feeding or Eating Disorder (UFED)
“I don’t know what’s wrong - I just know it’s hurting me.”
Sometimes, a person is clearly struggling with disordered eating - but their symptoms don’t fit neatly into any specific diagnostic box. They may restrict, binge, or purge, but not often enough, or not in a way that meets all the criteria for anorexia, bulimia, or binge eating disorder. In such cases, clinicians may use the diagnosis UFED.
What is UFED?
UFED stands for Unspecified Feeding or Eating Disorder. According to the DSM-5, this diagnosis is used when:
A person has clinically significant distress or impairment due to eating-related issues
But does not meet full diagnostic criteria for any specific feeding or eating disorder
And the clinician chooses not to specify why (e.g., due to lack of information in emergency or short-term settings)
UFED is not a “lesser” diagnosis. It is often used in:
Emergency rooms
Early stages of care
When symptoms are unclear or evolving
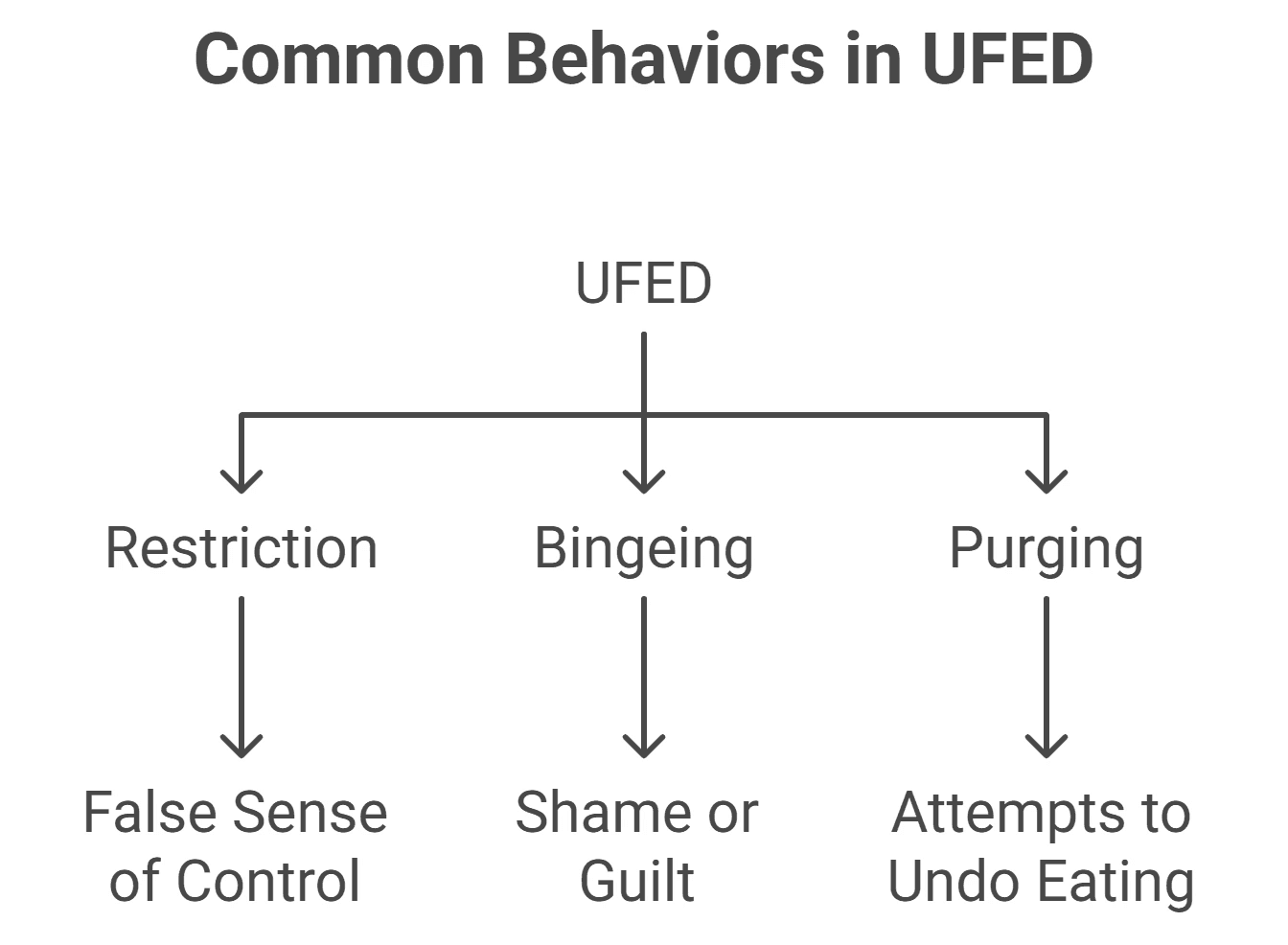
Common Behaviors Seen in UFED (Eating Disorder Hope):
Though not formally categorized, many people diagnosed with UFED experience a mix of the following:
Restriction: Extreme calorie control, sometimes consuming as little as 500 kcal/day. This can give a false sense of control, often seen in people with undiagnosed anorexia-like tendencies.
Bingeing: Secretive eating of large amounts of food, often to the point of discomfort, followed by shame or guilt. Unlike BED, this may happen less frequently.
Purging: Attempts to “undo” eating through vomiting, laxatives, or compulsive exercise - even after small or normal meals.
These behaviors can be just as dangerous as those seen in other eating disorders. People with UFED may feel invisible or invalidated, especially if they’re told they’re “not sick enough”. But their distress is real - and so is the need for support.
Pica
“My cravings don’t make sense - and I’m scared to talk about them.”
Pica is a feeding disorder marked by the persistent eating of non-food, non-nutritive substances - like chalk, soil, paper, hair, ice, or soap. While it might sound unusual, pica is more common than many realise, especially among children, pregnant women, and people with developmental or psychiatric conditions.
DSM-5 Diagnostic Criteria for Pica:
A. Persistent eating of non-nutritive, non-food substances for at least 1 month
B. The behavior is inappropriate for the individual’s developmental level
C. The behavior is not culturally supported (e.g., not part of ritual or traditional healing)
D. If it occurs with another condition (like autism, schizophrenia, or pregnancy), the behavior must be severe enough to warrant independent clinical attention
Who Experiences Pica?
Pica often co-occurs with:
Autism spectrum disorder
Intellectual disabilities
Schizophrenia
Pregnancy (particularly in cases of iron deficiency)
Childhood developmental delays
Why Does It Happen?
There’s no single cause, but common contributors include:
Nutritional deficiencies (especially iron or zinc)
Malnutrition
Sensory stimulation or soothing behavior in neurodivergent individuals
Cultural beliefs (in rare cases - but these are not considered disordered if culturally sanctioned)
Health Risks:
If left untreated, Pica can lead to:
Poisoning or toxicity (e.g., lead in paint or soil)
Gastrointestinal blockages
Dental damage
Parasitic infections
Why It’s Hard to Talk About:
Pica is deeply stigmatised. Many people feel embarrassed, confused, or ashamed by their cravings. But it’s important to remember:
Pica is not a moral failure or “weird habit”.
It’s a medical condition - and it’s treatable with compassion, proper diagnosis, and care.
Muscle Dysmorphia
“No matter how much I lift, I never feel big enough.”
While eating disorders are often seen through the lens of thinness, Muscle Dysmorphia flips the script. It’s a form of body dysmorphia where a person becomes obsessed with becoming more muscular, often at the cost of their physical and mental health. Though it can affect anyone, it’s especially common among men - and deeply embedded in gym culture and social media portrayals of the “ideal male body”.
What It Looks Like:
Constant worry about looking “small” or “weak”, even when muscular
Skipping social events, dates, or work to stick to workouts or meal plans
Intense guilt or anxiety after missing a workout
Excessive exercise routines, often causing injuries or chronic pain
Use of anabolic steroids or appearance-enhancing drugs, despite knowing the risks
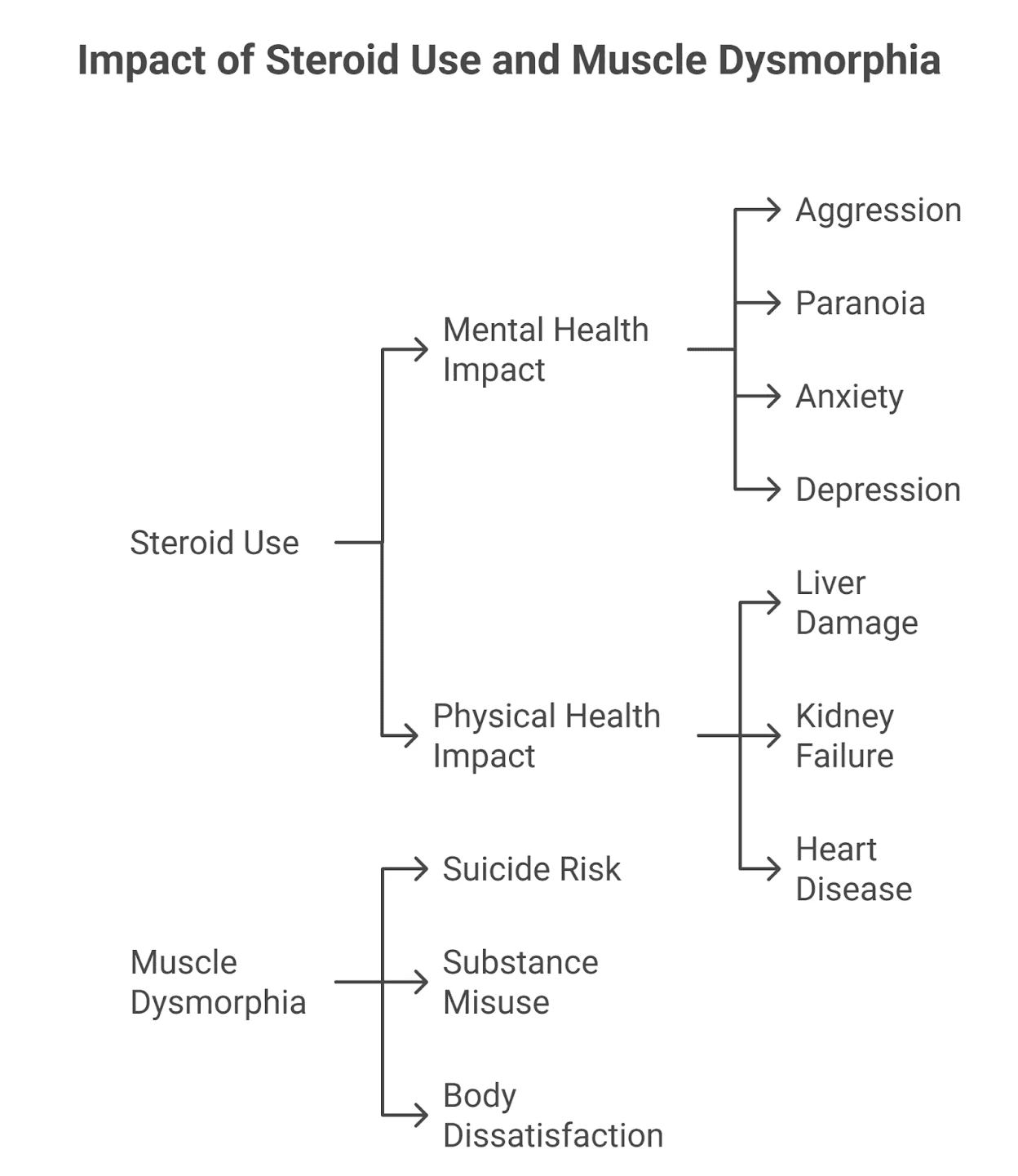
Health and Mental Health Impact:
According to the National Eating Disorders Association:
Steroid use can cause aggression, paranoia, anxiety, and depression
Long-term risks include liver damage, kidney failure, and heart disease
Muscle dysmorphia is associated with higher suicide risk, substance misuse, and severe body dissatisfaction
Cultural Context:
In Indian fitness culture, “bulking”, six-pack abs, and protein obsession can mask deep distress. The pressure to appear masculine and "fit" often prevents men from acknowledging that their behavior is disordered.
Muscle dysmorphia isn’t about vanity. It’s about feeling chronically not enough - and punishing your body to prove otherwise.
Orthorexia Nervosa
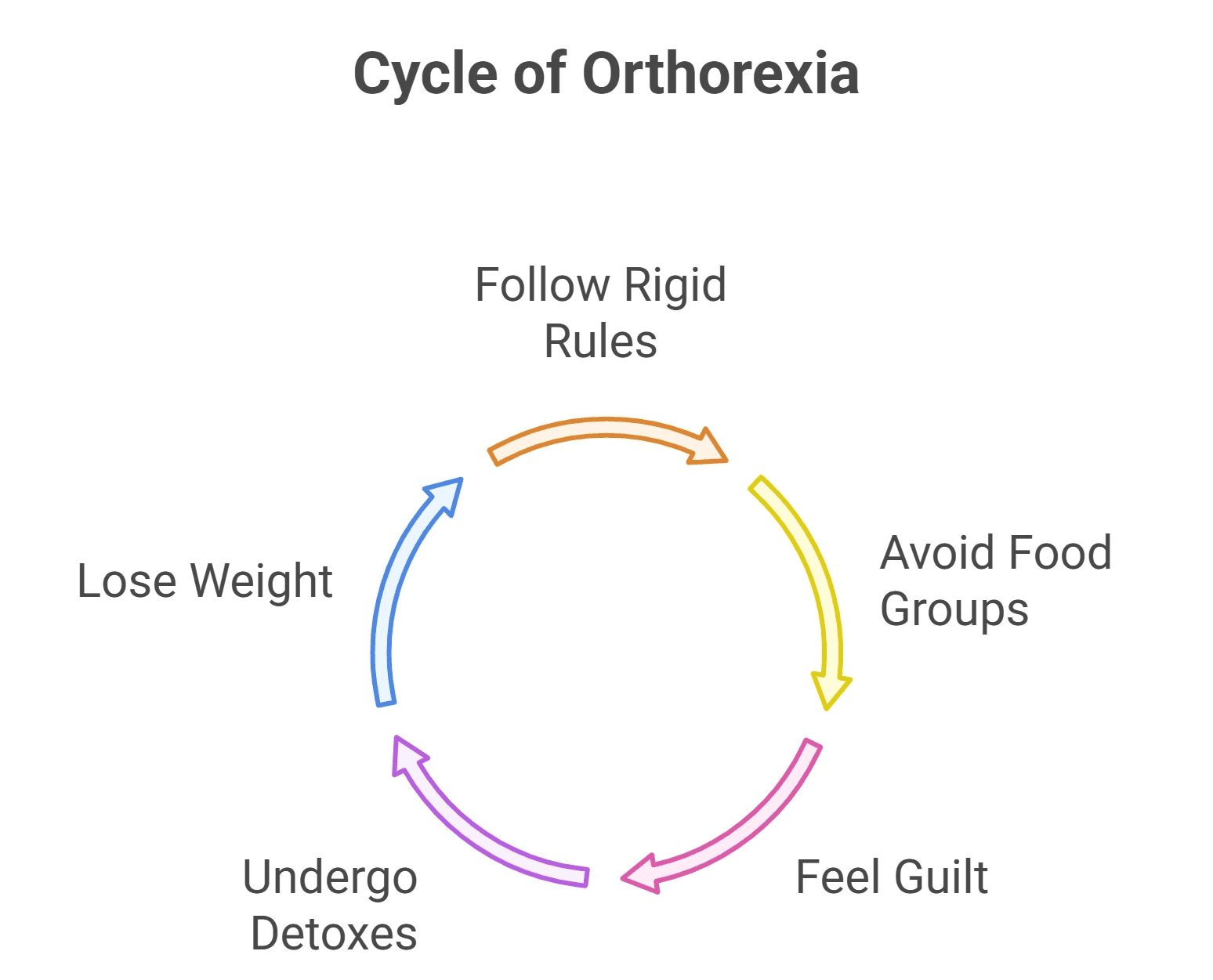
“I don’t want to eat anything that’s not clean.”
Orthorexia Nervosa isn’t officially recognized in the DSM-5 - but it’s rapidly emerging in clinical spaces, especially among wellness influencers, athletes, and health-conscious youth. While the pursuit of healthy eating might sound ideal, orthorexia goes further: it becomes an obsession with food purity that damages both health and life.
The term "orthorexia" was coined in 1997 by American physician Steve Bratman. Etymologically, it combines the Greek words "orthos" meaning "right", and "orexis" meaning "appetite". More accurately, however, the term is understood to mean "correct diet" in practice.
What Makes It Different?
Unlike anorexia or bulimia, orthorexia isn’t about weight - it’s about control, morality, and identity tied to “eating right”.
People with orthorexia:
Follow rigid “clean eating” rules
Avoid entire food groups (sugar, dairy, grains, oils, etc.)
Feel extreme guilt or shame after eating anything “impure”
May undergo frequent detoxes or cleanses
Lose weight unintentionally, but weight loss is not the primary goal
Proposed Diagnostic Criteria:
Criterion A: Obsessive focus on healthy eating, marked by:
Compulsive rules around what’s “good” and “bad” food
Emotional distress or shame when dietary rules are broken
Escalating restrictions over time (leading to weight loss or malnutrition)
Criterion B: These behaviors cause:
Physical complications (e.g., malnutrition, fatigue)
Social or academic disruptions (avoiding meals, events)
Self-worth becoming tied to adherence to the “clean” diet
The Emotional Cost:
Orthorexia is often praised in wellness spaces - but the person may be exhausted, isolated, and silently suffering. When “health” becomes punishment, something’s wrong.
In a world that glorifies clean eating, orthorexia hides in plain sight.
What Causes Eating Disorders?
There’s no single cause behind eating disorders - they emerge at the crossroads of biology, psychology, and culture. Often, what starts as a coping strategy slowly becomes a disorder. For many in India, it's not just about food or weight - it’s about control, fear, shame, and survival in a world that constantly comments on your body.
1. Biological Factors
Eating disorders have a strong genetic and neurobiological basis - they are not just a phase or a mindset.
A 2019 study found that anorexia nervosa shares genetic links with other mental health conditions like anxiety, depression, and OCD.
Behaviours like binge eating and vomiting have been found to be 46%–72% heritable.
First-degree relatives of those with anorexia or bulimia are 7 to 12 times more likely to have an eating disorder.
Brain chemicals like serotonin and dopamine - which regulate mood and reward - are often disrupted. This may contribute to binge eating, compulsive behaviors, and mood instability.
The gut-brain axis, still being studied, may also influence hunger signals, mood, and body image regulation.
Eating disorders are brain-based illnesses - not choices, not fads.
2. Psychological Factors
Certain personality traits and emotional patterns can increase vulnerability:
Perfectionism: A constant need to do things “right” - including eating, exercising, or looking a certain way.
Low self-esteem: Feeling “not enough” and using food or body control to gain a sense of worth.
History of trauma: Especially childhood abuse, bullying, or neglect.
Co-occurring disorders: Anxiety, depression, OCD, PTSD often exist alongside eating disorders.
3. Sociocultural Factors
In India, society's obsession with thinness, fairness, and control over women’s bodies often drives disordered patterns.
Bollywood & beauty filters reinforce unrealistic ideals of slimness and flawlessness.
Weight-focused parenting: Remarks like “don’t eat too much or you’ll get fat” are normalized.
Social media: Hashtags like #GlowUp and #WhatIEatInADay can quietly reinforce shame around natural bodies and appetites.
Marriage market pressure: Especially for women, there's an intense (often unspoken) need to appear “presentable” - slim, fair, and controlled.
Family policing: A girl who eats heartily or gains weight post-puberty is often seen as “undisciplined” or “problematic”.
Disordered eating isn’t always rebellion. Sometimes, it’s a desperate attempt to fit in, to be loved, to stay safe.
4. India-Specific Stressors
The cultural context here matters deeply.
Shame around normal body changes: Weight gain in PCOS, puberty, or pregnancy is treated like a flaw.
“Log kya kahenge” culture: The fear of judgment can push individuals to hide eating struggles - even from themselves.
Patriarchal norms: Strong women or those with bigger appetites may be mocked or judged - reinforcing the idea that a “controlled” woman is a “good” woman.
Signs & Symptoms: When to Seek Help
Eating disorders are not always visible. A person can seem “fine” while battling a war inside. Knowing the signs can help you or someone you love seek help early.
Emotional & Behavioral Signs
Obsession with food, weight, calories, or appearance
Avoiding meals or extreme meal-time anxiety
Secretive eating, hoarding, or hiding food
Feeling out of control around food
Using food to cope with emotions - bingeing, restricting, or purging
Distorted body image - never feeling “good enough”
Increased irritability, sadness, withdrawal, or mood swings
Physical Signs
Noticeable weight fluctuations (gain or loss)
Missed periods, low libido, or hormonal changes
Cold extremities, fatigue, dizziness, or fainting
Digestive issues, bloating, or food intolerance
Hair loss, dry skin, brittle nails
Brain fog and poor concentration
In Children:
Extreme pickiness that disrupts nutrition
Tantrums around meals
Sudden weight changes or refusal to eat entire food groups
Important: You don’t have to “look sick” to be struggling.
You don’t have to wait for things to get worse to seek support.
The Indian Silence: Why These Disorders Go Undiagnosed
In India, eating disorders often don’t look like what textbooks describe - and that’s exactly why they’re missed.
Despite growing awareness in urban spaces, the language, resources, and social permission to talk about disordered eating remain scarce.
1. No Words, No Language
In many Indian languages, there’s no direct translation for “eating disorder”. What might be anorexia is often brushed off as pet kam lagta hai (small appetite) or bimari ke baad kamzor ho gaya hai (she became weak after an illness).
Without the vocabulary, the suffering goes unnamed - and untreated.
2. Mistaken for “Discipline” or “Fasting”
Obsessive eating behaviours are frequently misread as virtues:
Skipping meals = good self-control
Avoiding carbs = fitness
Starving after festivals = cleansing
Culturally sanctioned practices like fasting during Navratri or Ramadan can sometimes overlap with disordered restriction - but intent matters. When control, fear, or guilt are the drivers, it’s no longer about faith or health.
3. Shame & Silence
Talking about food, body image, or mental health is still taboo in many households. For girls, expressing discomfort with body changes is often silenced with, “Sabko hota hai. Adjust karna padta hai”.
For boys, admitting to body dissatisfaction is often mocked: “Why do you care so much? Are you a model?”
The result? Shame becomes silence. Silence becomes suffering.
4. Gendered Expectations
Eating disorders affect all genders - but men are less likely to be diagnosed. Why? Because Indian masculinity often discourages emotional vulnerability and body talk.
Men with muscle dysmorphia or binge eating are more likely to be praised for their gym routines than to be seen as struggling.
5. Lack of Trained Professionals
In Tier 2 and Tier 3 cities, access to mental health professionals trained in eating disorders is rare. Even in metros, most therapists don’t receive specialised ED training, and medical professionals often miss the signs unless weight loss is extreme.
The danger is not just the disorder - it’s the silence that hides it.
Breaking that silence is the first step toward healing.
Long-Term Effects If Left Untreated
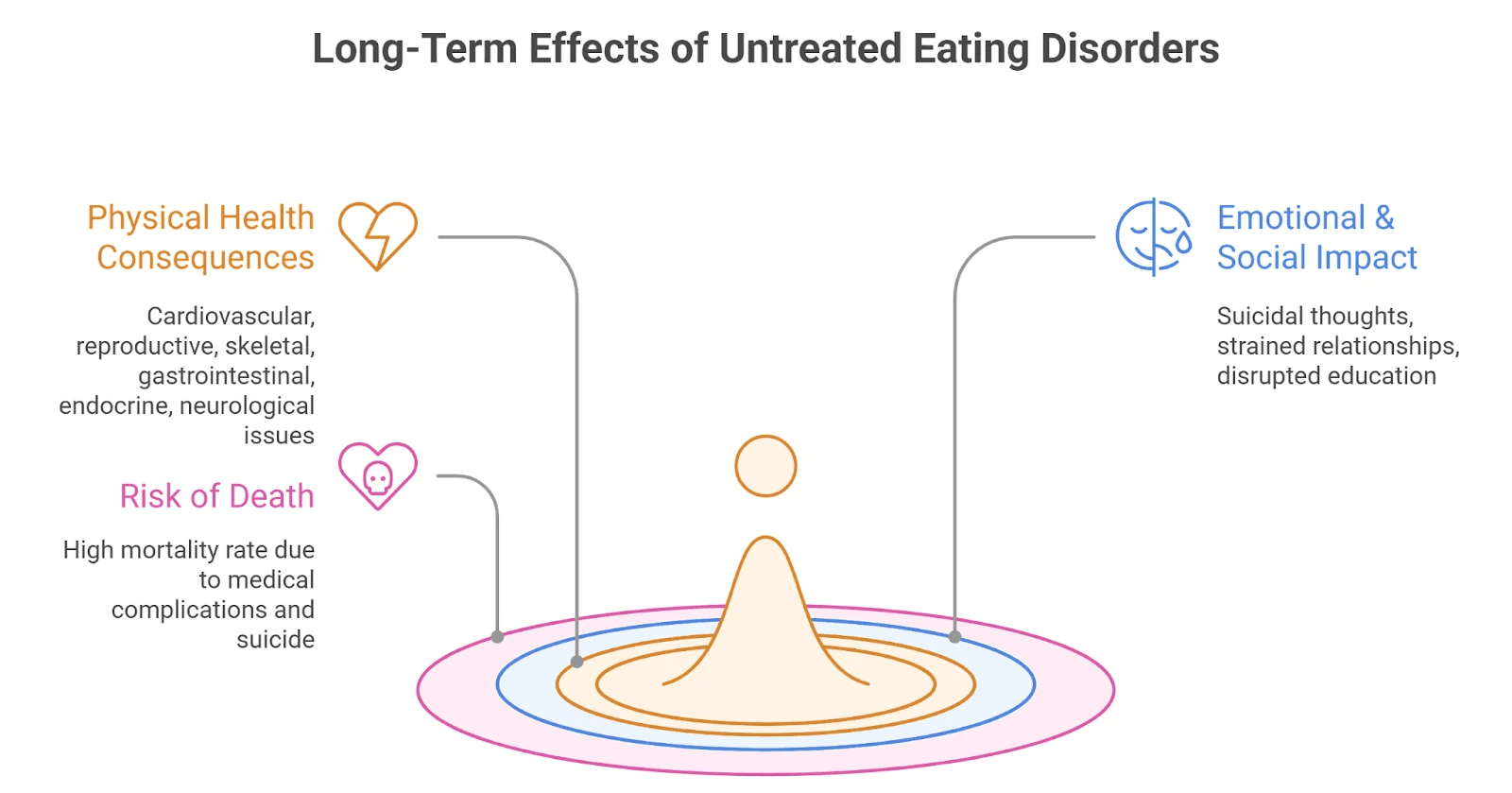
Eating disorders are not a phase. They are serious, progressive, and - without help - can lead to long-term harm across every system in the body.
1. Physical Health Consequences
Cardiovascular: Low heart rate, irregular heartbeat, heart failure
Reproductive: Missed periods, infertility, miscarriage risk
Skeletal: Bone thinning, early-onset osteoporosis
Gastrointestinal: Acid reflux, chronic constipation, damaged intestines
Endocrine: Hormonal imbalance, anemia, insulin resistance
Neurological: Poor concentration, memory issues, seizures
Electrolyte imbalances: Can lead to sudden cardiac arrest
Research shows that women who have struggled with eating disorders in the past often face long-term ripple effects. As adults, they are more likely to remain underweight, struggle with depression, smoke, or postpone childbirth. Many also experience complications during pregnancy - including severe nausea, unexplained bleeding, miscarriages, or even the need for medically induced abortions.
Another body of research links long-term undernourishment, especially in adolescents with anorexia, to lasting health issues such as stunted growth, fertility problems, and weakened bones due to early-onset osteoporosis.
2. Emotional & Social Impact
Suicidal thoughts & self-harm are common, especially in bulimia and anorexia
Strained friendships and family relationships
Disrupted education or career paths
Chronic low self-worth and emotional numbness
Isolation - not just from people, but from joy
3. Risk of Death
Eating disorders have a very high mortality rate among all mental health conditions - due to medical complications and suicide.
Getting help early can save a life - and restore one.
It’s never “too soon” or “not serious enough” to reach out.
Treatment That Heals Beyond Food
Eating disorders are not just about food - so recovery must reach far beyond the plate. True healing involves rewiring beliefs, emotions, and behaviors that have taken root over years. It’s about learning to live again, not just eat again.
Therapies That Work
1. CBT-E (Enhanced Cognitive Behavioral Therapy)
CBT-E is one of the most evidence-backed treatments for eating disorders across diagnoses. It helps people challenge distorted thoughts around food, weight, and self-worth, and establish regular, nourishing eating patterns.
The treatment typically progresses in four stages - as broken down by CBT-E Org:
Stage 1 focuses on understanding the eating problem and building structure around food.
Stage 2 is a brief review period to evaluate progress.
Stage 3 targets the root causes - like fear of weight gain, rigid rules, and emotional regulation.
Stage 4 prepares the person to maintain progress, prevent relapse, and move forward with life.
For underweight individuals, the process may include 40 sessions over 40 weeks, with a careful, collaborative approach to weight restoration.
2. DBT (Dialectical Behavior Therapy)
Originally developed for Borderline Personality Disorder (BPD), DBT is highly effective for eating disorders that involve emotional dysregulation - like bingeing or purging in response to distress.
A 12-month study showed that DBT significantly reduced both eating disorder and BPD symptoms, especially by improving coping skills. This approach teaches distress tolerance, emotion regulation, and interpersonal effectiveness - tools that many people with EDs never had the chance to build.
3. Family-Based Therapy (FBT)
FBT empowers caregivers - especially in adolescents - to take an active role in refeeding and recovery. It’s not about blame; it’s about building a support system that the eating disorder can’t thrive in.
FBT has shown strong success in treating anorexia and bulimia in children and teens, and is increasingly adapted for ARFID and atypical presentations as well.
4. Schema Therapy
For individuals who carry deep-rooted beliefs like “I am only lovable if I’m thin” or “I must be in control to be safe”, schema therapy can be life-changing. It targets these long-standing patterns and helps people rebuild a more compassionate relationship with themselves.
5. Psychoanalytic Therapy
While slower-paced, this approach is helpful for those whose eating disorders are closely tied to trauma, early attachment issues, or identity conflicts. It allows space to explore not just behavior, but the unconscious pain underneath it.
6. Nutrition Counseling
With the help of a trained dietitian who understands eating disorders, individuals learn to rebuild trust in hunger cues, challenge food fears, and create a balanced relationship with eating. It’s not about dieting - it’s about nourishing body and mind.
7. Medication
While not a standalone treatment, medications may help manage co-occurring conditions like depression, anxiety, or OCD - which often coexist with eating disorders and can make recovery harder without support.
Prevention & Healing at Home: Building Food Peace Early
Eating disorders often begin quietly - in subtle restrictions, anxious meal times, or offhand comments about weight. But with mindful habits and language, homes can become places of prevention, not pressure.
Whether you or your loved ones are struggling, or simply want to foster a healthier environment, here are everyday tools that nourish both body and mind:
Practice Mindful Eating
Eat slowly, without screens. Learn to listen to your body’s cues - hunger, fullness, satisfaction - instead of rushing through meals or ignoring discomfort.Body Neutrality Over Body Judgment
Shift from asking “Do I look good?” to “How do I feel today?” Appreciate your body for what it can do - digest, dance, carry you through life - not just how it looks.Challenge Diet Talk
Replace “good food vs bad food” with “all foods fit”. Labeling foods morally often creates guilt and shame that fuel disordered eating.Support Regular Meals
Predictable eating patterns help stabilize energy, emotions, and appetite. It’s not about being rigid - it’s about offering safety through rhythm.Celebrate Cultural Foods Without Guilt
Indian food traditions are inherently nurturing. Whether it’s khichdi for gut comfort, curd for cooling, or ghee for strength - there’s healing in heritage.Move for Joy, Not Punishment
Redefine movement: a morning walk, dancing to your favorite song, stretching at night. Let it feel like care, not compensation.Foster Open Conversations
Don’t wait for a crisis. Create non-judgmental spaces where body image, mental health, and identity can be spoken about - and heard with care.
Urging a Loved One to Seek Help (With Compassion)
When someone you care about is struggling, it’s natural to feel helpless or unsure of what to say. But the right words, tone, and timing can plant seeds for healing.
Don’t blame or accuse.
Instead of “Why are you doing this to yourself?” try:
“I’ve noticed you seem really anxious around food lately. I’m here if you ever want to talk.”Offer support, not solutions.
Try: “Would you like me to help you look for someone to talk to?” or “We can figure this out together.”Avoid comments on appearance.
Even praise like “You look healthier now!” can be misunderstood. Focus on how they feel, not how they look.Be patient.
Denial is common - not from deceit, but from fear or shame. Keep showing up without pressure.Encourage professional help.
Healing requires trained support - not just willpower or home remedies.
Recovery Is Not Linear
It’s filled with steps forward and steps back. But what matters is showing up again, and again. You don’t have to be “sick enough” to deserve help. You just have to begin.
How Are Eating Disorders Diagnosed?
Many people don’t recognize they’re struggling - or they hide it out of fear. But early diagnosis can prevent years of suffering and even save lives.
Step 1: Consult a Doctor or Mental Health Professional
Start by speaking with someone you trust - a therapist, psychiatrist, or even a primary care doctor.
Step 2: Medical Assessments
These help rule out physical complications and nutritional deficiencies:
Weight and height monitoring
Vital signs: blood pressure, heart rate
Blood and urine tests to evaluate electrolytes, hormones, liver and kidney function
Step 3: Psychological Evaluations
Clinical interviews exploring food behaviors, beliefs, and emotional history
Self-report tools like the Eating Disorder Examination Questionnaire (EDE-Q) or SCOFF
Assessment of co-occurring issues like anxiety, depression, trauma, or OCD
An official diagnosis is typically made using DSM-5-TR criteria, but even without a label, the need for care is valid. If food and body thoughts are interfering with daily life - help is not only allowed, it’s essential.
Spotlight: Hidden Eating Disorders in Indian Culture
Eating disorders in India don’t always scream for attention. They whisper - through rituals of discipline, wellness, and control.
The bride who fasts obsessively before her wedding, so she can “look perfect” in photos - even if it means fainting during fittings.
The gym bro who spirals into panic if he misses a workout, afraid his “gains” will disappear overnight.
The diabetic teen who eats painfully “clean”, not out of health, but fear - of judgment, stigma, and being seen as undisciplined.
The working mother who skips meals just to feel a shred of control in her chaotic day - praised as “strong” but silently starving.
The young woman who avoids eating out with friends to stay “pure” on her diet - believing one slip ruins everything.
These stories don’t always come with a diagnosis. They don’t always look like illness.
But they carry the same pain - and they deserve the same care.
How Elfina Can Help
At Elfina, we understand that eating disorders are more than food or weight. They’re woven into emotions, identity, family roles, and cultural pressures.
That’s why our care is holistic, empathetic, and culturally attuned:
🎓 Trained Experts: Work with licensed therapists who specialize in eating disorders, body image, and co-occurring mental health concerns like anxiety, trauma, or OCD.
🪞 Contextual Therapy: Our therapists understand the Indian context - fatphobia, “log kya kahenge”, generational body shame, and perfectionism.
🧠 Integrated Support: Our team includes both mental health professionals and nutrition specialists - because healing isn’t just mental or physical. It’s both.
🤝 At Your Pace: Whether you're ready for deep work or just starting to explore your relationship with food, Elfina meets you where you are - with compassion, not pressure.
🔒 Confidential & Accessible: 100% online, confidential, and available no matter your location or stage of struggle.
🌟 94% of clients are matched with a suitable therapist on the first try.
🌟 80%+ of our therapists have 5+ years of clinical experience.

Whether you’re surviving in silence, supporting a loved one, or just wondering if something is off - you are not alone.
Elfina is here to walk with you toward food freedom, self-trust, and emotional healing.
Frequently Asked Questions (FAQs)
Can you recover from an eating disorder without therapy?
Some people make progress through self-help, supportive communities, or personal insight - but for most, therapy is essential. Eating disorders are deeply rooted in thoughts, emotions, and behaviors. A trained therapist can help unpack the “why” behind disordered patterns and support long-term healing.
Do men have eating disorders?
Absolutely. While underdiagnosed, eating disorders affect people of all genders. Muscle dysmorphia, compulsive exercise, and binge eating often show up differently in men - and may be overlooked due to stigma or cultural expectations around masculinity.
Is fasting for religious reasons considered disordered eating?
Not necessarily. But it can become disordered when religious fasting is used to mask restriction or control weight.
A study in the Journal of Eating Disorders found that religious participants who altered their eating for both spiritual and weight-control reasons experienced greater disordered eating and appearance-related pressure than those who didn’t change their diet.
What if I don’t feel “sick enough”?
There is no such thing as not being “sick enough” to deserve help.
Eating disorders are mental illnesses, not defined by appearance or weight. If your thoughts, habits, or emotions around food cause distress - you deserve care.
How do I talk to my child if I suspect they have an eating disorder?
Start with gentle concern, not confrontation. Try:
“I’ve noticed some changes and I care about how you’re feeling - can we talk about it?”
Avoid comments about appearance. Instead, focus on emotions, stress, or behaviors. Consider reaching out to a therapist for support - for them, and for you.
Conclusion: Food Is Not the Enemy. Shame Is.
Eating disorders are not vanity.
They are not weakness.
They are not something you can simply “snap out of”.
They are often a quiet cry for control, connection, and peace - disguised as food rules, skipped meals, or relentless self-criticism.
You are not “too much”.
You are not “too dramatic”.
You are not “too far gone”.
You deserve joy. Nourishment. A relationship with food that feels safe - not punishing.
At Elfina, we believe recovery is not about perfection. It’s about coming home to yourself.
Whether you’re noticing the first signs or have lived with this struggle for years - it’s not too late. It’s not too mild. And it’s definitely not your fault.
Elfina’s therapists and nutrition specialists are here to walk with you - with empathy, cultural understanding, and clinical care.
Healing is possible. You don’t have to do it alone.


It’s Not Always About the Food: Understanding, Treating & Healing from Eating Disorders
|
13
min read
|
Tanvi
It’s Not Always About the Food
A college student becomes obsessed with “clean eating”. No sugar, no oil, no dinners out. She’s praised for her discipline - until she stops showing up altogether.
A teenage boy spends hours at the gym and is flooded with likes on his shirtless photos. No one sees the binge–guilt–starve cycle he’s stuck in.
These aren’t stories of vanity.
They’re stories of control, shame, and a quiet desperation to feel okay.
Myth: You can “see” an eating disorder
Reality: Many eating disorders don’t look like what we expect. They don’t always involve extreme thinness.
They can hide behind:
“Wellness” routines
Intermittent fasting
Gym obsession
“Good discipline”
In India especially, we mistake early signs for self-control. We compliment the person who skips meals, praises khichdi and lemon water, or fasts even when exhausted.
But suffering doesn’t always look sick.
What the data says
A 2018 study in Mysore found that over 26% of students showed signs of disordered eating.
In Bangalore, 66% of psychiatrists had seen at least one eating disorder case in the past year.
Cultural factors - like peer pressure, appearance-based marriage markets, and weight-related comments - often play a hidden but powerful role.
Despite rising cases, India still lacks comprehensive national data on eating disorders - a silence that’s part of the problem.
What Are Eating Disorders?
Eating disorders are not diets gone wrong.
They are serious, diagnosable mental health conditions that impact how people eat, think, feel, and function.
Clinical definition (DSM-5-TR):
“A persistent disturbance of eating or eating-related behaviour that results in the altered consumption or absorption of food and that significantly impairs physical health or psychosocial functioning.”
This could mean:
Restricting food out of fear
Binge eating until numb
Obsessively “eating clean”
Feeling deep guilt after every meal
It’s not a phase or a choice
It’s not about vanity.
It’s about coping - with trauma, low self-worth, control issues, or anxiety.
And it can affect anyone - regardless of gender, age, caste, body size, or income.
Still, in India, many go undiagnosed - either due to stigma or lack of awareness, even among professionals.
Types of Eating Disorders
Eating disorders are not just about food - they are about pain, identity, control, and how that pain gets expressed through eating patterns, rituals, or avoidance. These conditions can look vastly different across people and cultures. One person may be severely restricting calories; another might binge in secret and live in shame; a third may obsess over "clean eating" while slowly disappearing into anxiety.
The DSM-5-TR (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision) currently outlines eight clinically recognised feeding and eating disorders, each with distinct diagnostic criteria and severity levels. These include Anorexia Nervosa, Bulimia Nervosa, Binge Eating Disorder, ARFID, Rumination Disorder, Pica, Other Specified Feeding or Eating Disorders (OSFED), and Unspecified Feeding or Eating Disorders.
In this section, we’ll explore each of these diagnoses using the DSM-5’s official diagnostic criteria - alongside lived realities, emerging research, and cultural factors that shape how eating disorders show up, especially in Indian contexts.
Anorexia Nervosa
"I’m not thin enough. I’m never thin enough."
Anorexia isn’t about vanity - it’s often about control in a world that feels chaotic.
People with anorexia engage in extreme restriction, fuelled by a distorted body image and an intense fear of gaining weight.
Diagnostic Criteria (DSM-5):
A. Restriction of energy intake leading to significantly low body weight (relative to age, sex, developmental stage, and health).
B. Intense fear of gaining weight or persistent behaviour that prevents weight gain - even when underweight.
C. Distorted body image or an inability to recognise the seriousness of current low weight.
Subtypes (as per Eating Disorder Resources):
Restricting Type: Weight loss achieved through strict dieting, fasting, or excessive exercise.
Binge-Eating/Purging Type: Regular episodes of binge eating or purging (vomiting, laxatives) while still maintaining a significantly low weight.
Important: A person does not need to be underweight to be diagnosed with anorexia. Larger-bodied individuals can still meet all other criteria - but often go undiagnosed due to cultural weight stigma.
Remission Specifiers:
Partial Remission: Weight has returned to a healthier level, but fear of weight gain or body image issues remain.
Full Remission: No criteria have been met for a sustained period.
Levels of Severity (as per AAFP):
Severity | BMI Range |
Mild | ≥ 17 kg/m² |
Moderate | 16–16.99 kg/m² |
Severe | 15–15.99 kg/m² |
Extreme | < 15 kg/m² |
Diagnostic Crossovers:
A landmark study found that most women with anorexia transitioned between subtypes over time - and some shifted to bulimia before often reverting back to anorexia. This tells us how fluid and complex eating disorders can be.
Pop Culture Reference:
Nina in Black Swan - driven by perfection, fear, and control - reflects the haunting emotional world of someone with anorexia.
Bulimia Nervosa
“I binge until I feel numb - then I punish myself.”
Bulimia often hides behind smiling faces and “normal” bodies.
It involves cycles of binge eating, followed by compensatory behaviors like vomiting, excessive exercise, or starvation.
Diagnostic Criteria (DSM-5):
A. Recurrent episodes of binge eating. Each episode involves:
Eating an amount of food larger than typical in a short time (e.g., 2 hours)
Feeling out of control during the episode
B. Recurrent inappropriate compensatory behaviors to prevent weight gain - such as vomiting, laxatives, fasting, or over-exercising.
C. These behaviors occur at least once a week for 3 months.
D. Self-worth is disproportionately influenced by body shape and weight.
E. The disturbance doesn’t occur exclusively during episodes of anorexia nervosa.
Levels of Severity (as per AAFP):
Severity | Episodes of compensatory behavior per week |
Mild | 1–3 episodes |
Moderate | 4–7 episodes |
Severe | 8–13 episodes |
Extreme | 14+ episodes |
Health Consequences (if untreated):
According to Psych Central, untreated bulimia can affect nearly every system:
Cardiovascular: Irregular heartbeat, heart failure
Gastrointestinal: Esophageal damage, pancreatitis, constipation
Endocrine: Anemia, menstrual issues, insulin resistance
Neurological: Brain fog, seizures, sleep issues, stroke
When It Begins - and Who It Affects:
According to the Children’s Hospital of Philadelphia, bulimia most often begins in adolescence or early adulthood. It’s more common in girls than boys, but it can affect people of any gender.
Despite its often-invisible presentation, bulimia carries a high emotional and physical toll, and in some cases, a higher risk of suicide than anorexia nervosa due to intense depressive symptoms and self-loathing.
What Binges Look Like:
Binges often involve high-calorie foods people normally restrict - sweets, fried foods, bread. It’s not hunger; it’s emotional overwhelm, followed by purging to feel in control again.
Real-Life Reference:
Princess Diana openly shared her struggles with bulimia - breaking silence in a world that often rewards appearance and ignores inner pain.
Binge Eating Disorder (BED)
“Sometimes I eat until I feel sick - and then I cry in shame.”
Binge Eating Disorder (BED) is one of the most common but misunderstood eating disorders. Unlike bulimia, there are no compensatory behaviors like purging or over-exercising. And unlike anorexia, weight loss is not a defining feature. At its core, BED is about losing control around food, feeling immense guilt afterward, and falling into a cycle of emotional distress.
Many people with BED appear to function “normally” in daily life - going to work, raising families, meeting deadlines - while battling overwhelming episodes of binge eating in private. It's not simply “overeating” or “laziness”. It’s a mental health condition rooted in emotion regulation, trauma, and often years of dieting or shame.
DSM-5 Diagnostic Criteria for Binge Eating Disorder:
A. Recurrent episodes of binge eating. Each episode is defined by both:
Eating, in a short period (e.g., 2 hours), an amount of food significantly larger than most people would eat under similar circumstances.
A sense of lack of control during the episode.
B. Binge-eating episodes are associated with at least three of the following:
Eating much more rapidly than normal
Eating until uncomfortably full
Eating large amounts when not physically hungry
Eating alone due to embarrassment
Feeling disgusted, depressed, or very guilty afterward
C. Marked distress regarding binge eating.
D. The behavior occurs at least once a week for three months.
E. The binge eating is not associated with compensatory behaviors (i.e., not bulimia or anorexia).
Severity Levels (as per PsychDB):
Severity | Episodes of binge eating per week |
Mild | 1–3 episodes |
Moderate | 4–7 episodes |
Severe | 8–13 episodes |
Extreme | 14+ episodes |
Emotional and Developmental Roots:
BED isn’t just about food - it’s about feelings. Many people report early childhood struggles, such as:
Emotional trauma, family conflict, or parental mental illness
Childhood obesity and body shaming
Negative perfectionism or feeling “never good enough”
A history of being told to “control” one’s appetite or weight
Physical or sexual abuse
Psychologically, negative affectivity, low self-worth, and a history of loss of control eating in childhood are common precursors.
In Remission:
Partial remission: Binge eating occurs less than once per week for a sustained period
Full remission: No binge episodes or distress for a sustained period
Avoidant/Restrictive Food Intake Disorder (ARFID)
“I’m not scared of gaining weight - I’m scared of eating at all.”
ARFID is a lesser-known but serious eating disorder that’s not driven by body image concerns. Instead, individuals with ARFID struggle with extreme food avoidance - often because of sensory aversions, lack of interest in food, or fear of choking, vomiting, or discomfort.
This condition is often mistaken for “just picky eating”, especially in children, but the consequences can be severe - from malnutrition and stunted growth to social isolation and emotional distress.
DSM-5 Diagnostic Criteria for ARFID:
A. An eating or feeding disturbance (e.g., apparent lack of interest in eating or food; avoidance based on sensory characteristics of food; fear of aversive consequences of eating) manifested by persistent failure to meet nutritional or energy needs, associated with one or more of the following:
Significant weight loss (or failure to gain weight or grow as expected)
Significant nutritional deficiency
Dependence on nutritional supplements or tube feeding
Marked interference with psychosocial functioning
B. The disturbance is not due to food unavailability or culturally sanctioned practices (e.g., religious fasting).
C. The eating disturbance is not due to body image issues - differentiating it from anorexia or bulimia.
D. If occurring alongside another medical or mental condition, the severity of eating disturbance must be clinically significant and beyond what’s typical for that condition.
What ARFID Can Look Like:
A child who refuses to eat anything but plain white rice or biscuits
A teen who fears vomiting after a past choking incident
An adult who lives on protein shakes due to strong taste or texture aversions
There are three common subtypes of ARFID:
Sensory-based avoidance (due to smell, texture, taste)
Fear-based restriction (fear of choking, vomiting, etc.)
Appetite-based restriction (very low hunger or interest in food)
Medical Consequences:
As per clinical literature, untreated ARFID can lead to:
Nutritional deficiencies (iron, calcium, vitamins)
Electrolyte imbalances
Bradycardia (slow heart rate), fainting
Gastrointestinal issues, bone loss
Amenorrhea (loss of menstruation in those assigned female at birth)
Important to Know:
ARFID is not “just a phase” or something people “grow out of”. Children who don’t outgrow early picky eating - or who experience trauma related to food - may develop ARFID, and the condition often continues into adolescence or adulthood if untreated.
Other Specified Feeding or Eating Disorders (OSFED)
“I’m not ‘sick enough’ to count - but I’m still suffering.”
Not every eating disorder fits into a neat clinical box. In real life, people often display serious, even dangerous, symptoms - but don’t meet the full criteria for anorexia, bulimia, or binge eating disorder. That’s where OSFED comes in.
OSFED stands for Other Specified Feeding or Eating Disorders, and it’s the most commonly diagnosed eating disorder in many countries, including India. Cultural masking - like calling disordered patterns “good discipline”, “fasting”, or “clean living” - can obscure how severe the struggle really is.
DSM-5 Definition:
OSFED is diagnosed when someone experiences clinically significant symptoms of a feeding or eating disorder, but the presentation doesn’t meet the full diagnostic criteria for other eating disorders.
Importantly, OSFED is not “less serious”. A meta-analysis found that adolescents with OSFED were just as likely to be hospitalized as those with anorexia nervosa.
Subtypes of OSFED (DSM-5):
Atypical Anorexia Nervosa
All criteria for anorexia nervosa are met, except the person is not underweight. This is especially common in India, where people in higher-weight bodies may be overlooked or even encouraged to continue restrictive eating.Bulimia Nervosa (Low Frequency/Duration)
Meets all bulimia criteria, but bingeing and purging occur less than once a week or for less than 3 months.Binge Eating Disorder (Low Frequency/Duration)
Binge episodes happen less frequently or for a shorter period, but still cause significant distress.Purging Disorder
Regular purging (vomiting, laxatives, etc.) without bingeing.Night Eating Syndrome
Repeatedly eating after waking from sleep or consuming excessive food post-dinner, with full awareness. This causes significant distress and is not due to lifestyle, cultural norms, or other medical conditions.
Why It’s So Common in India:
Many people fast for religious or “discipline” reasons - masking harmful patterns
Weight stigma can lead people in larger bodies to go undiagnosed
Cultural silence around food, appearance, and distress makes it harder to name the issue
Individuals with OSFED may feel like they’re “not sick enough” to deserve help - but they are.
Rumination Disorder
“I keep regurgitating my food - I don’t know why, and I feel ashamed.”
Rumination Disorder may sound unusual, but it’s a real and serious condition - characterised by repeated regurgitation of food, which may be re-chewed, re-swallowed, or spit out. It’s not due to nausea or a medical problem like reflux. And while it’s more common in infants and people with developmental disabilities, it can occur in adults too.
Often dismissed as “weird” or mistaken for a physical issue, Rumination Disorder can lead to malnutrition, weight loss, dental erosion, electrolyte imbalances, and emotional distress if left untreated.
DSM-5 Diagnostic Criteria:
A. Repeated regurgitation of food over a period of at least 1 month. This may include re-chewing, re-swallowing, or spitting the food out.
B. The behavior is not due to a medical condition like gastroesophageal reflux or pyloric stenosis.
C. The disturbance does not occur exclusively during anorexia, bulimia, BED, or ARFID.
D. If it occurs alongside a neurodevelopmental condition (e.g., intellectual disability), the behavior is severe enough to warrant clinical attention.
Why It’s Misunderstood:
People may hide it out of embarrassment
It can be misdiagnosed as reflux, nausea, or vomiting
In adults, especially, it's often ignored or wrongly classified
Important Clarification:
While Rumination Disorder is listed separately from OSFED in the DSM-5, some clinicians may include it under the OSFED umbrella in practical contexts - especially when the presentation doesn’t fully meet criteria or co-occurs with other disordered eating behaviors.
Unspecified Feeding or Eating Disorder (UFED)
“I don’t know what’s wrong - I just know it’s hurting me.”
Sometimes, a person is clearly struggling with disordered eating - but their symptoms don’t fit neatly into any specific diagnostic box. They may restrict, binge, or purge, but not often enough, or not in a way that meets all the criteria for anorexia, bulimia, or binge eating disorder. In such cases, clinicians may use the diagnosis UFED.
What is UFED?
UFED stands for Unspecified Feeding or Eating Disorder. According to the DSM-5, this diagnosis is used when:
A person has clinically significant distress or impairment due to eating-related issues
But does not meet full diagnostic criteria for any specific feeding or eating disorder
And the clinician chooses not to specify why (e.g., due to lack of information in emergency or short-term settings)
UFED is not a “lesser” diagnosis. It is often used in:
Emergency rooms
Early stages of care
When symptoms are unclear or evolving
Common Behaviors Seen in UFED (Eating Disorder Hope):
Though not formally categorized, many people diagnosed with UFED experience a mix of the following:
Restriction: Extreme calorie control, sometimes consuming as little as 500 kcal/day. This can give a false sense of control, often seen in people with undiagnosed anorexia-like tendencies.
Bingeing: Secretive eating of large amounts of food, often to the point of discomfort, followed by shame or guilt. Unlike BED, this may happen less frequently.
Purging: Attempts to “undo” eating through vomiting, laxatives, or compulsive exercise - even after small or normal meals.
These behaviors can be just as dangerous as those seen in other eating disorders. People with UFED may feel invisible or invalidated, especially if they’re told they’re “not sick enough”. But their distress is real - and so is the need for support.
Pica
“My cravings don’t make sense - and I’m scared to talk about them.”
Pica is a feeding disorder marked by the persistent eating of non-food, non-nutritive substances - like chalk, soil, paper, hair, ice, or soap. While it might sound unusual, pica is more common than many realise, especially among children, pregnant women, and people with developmental or psychiatric conditions.
DSM-5 Diagnostic Criteria for Pica:
A. Persistent eating of non-nutritive, non-food substances for at least 1 month
B. The behavior is inappropriate for the individual’s developmental level
C. The behavior is not culturally supported (e.g., not part of ritual or traditional healing)
D. If it occurs with another condition (like autism, schizophrenia, or pregnancy), the behavior must be severe enough to warrant independent clinical attention
Who Experiences Pica?
Pica often co-occurs with:
Autism spectrum disorder
Intellectual disabilities
Schizophrenia
Pregnancy (particularly in cases of iron deficiency)
Childhood developmental delays
Why Does It Happen?
There’s no single cause, but common contributors include:
Nutritional deficiencies (especially iron or zinc)
Malnutrition
Sensory stimulation or soothing behavior in neurodivergent individuals
Cultural beliefs (in rare cases - but these are not considered disordered if culturally sanctioned)
Health Risks:
If left untreated, Pica can lead to:
Poisoning or toxicity (e.g., lead in paint or soil)
Gastrointestinal blockages
Dental damage
Parasitic infections
Why It’s Hard to Talk About:
Pica is deeply stigmatised. Many people feel embarrassed, confused, or ashamed by their cravings. But it’s important to remember:
Pica is not a moral failure or “weird habit”.
It’s a medical condition - and it’s treatable with compassion, proper diagnosis, and care.
Muscle Dysmorphia
“No matter how much I lift, I never feel big enough.”
While eating disorders are often seen through the lens of thinness, Muscle Dysmorphia flips the script. It’s a form of body dysmorphia where a person becomes obsessed with becoming more muscular, often at the cost of their physical and mental health. Though it can affect anyone, it’s especially common among men - and deeply embedded in gym culture and social media portrayals of the “ideal male body”.
What It Looks Like:
Constant worry about looking “small” or “weak”, even when muscular
Skipping social events, dates, or work to stick to workouts or meal plans
Intense guilt or anxiety after missing a workout
Excessive exercise routines, often causing injuries or chronic pain
Use of anabolic steroids or appearance-enhancing drugs, despite knowing the risks
Health and Mental Health Impact:
According to the National Eating Disorders Association:
Steroid use can cause aggression, paranoia, anxiety, and depression
Long-term risks include liver damage, kidney failure, and heart disease
Muscle dysmorphia is associated with higher suicide risk, substance misuse, and severe body dissatisfaction
Cultural Context:
In Indian fitness culture, “bulking”, six-pack abs, and protein obsession can mask deep distress. The pressure to appear masculine and "fit" often prevents men from acknowledging that their behavior is disordered.
Muscle dysmorphia isn’t about vanity. It’s about feeling chronically not enough - and punishing your body to prove otherwise.
Orthorexia Nervosa
“I don’t want to eat anything that’s not clean.”
Orthorexia Nervosa isn’t officially recognized in the DSM-5 - but it’s rapidly emerging in clinical spaces, especially among wellness influencers, athletes, and health-conscious youth. While the pursuit of healthy eating might sound ideal, orthorexia goes further: it becomes an obsession with food purity that damages both health and life.
The term "orthorexia" was coined in 1997 by American physician Steve Bratman. Etymologically, it combines the Greek words "orthos" meaning "right", and "orexis" meaning "appetite". More accurately, however, the term is understood to mean "correct diet" in practice.
What Makes It Different?
Unlike anorexia or bulimia, orthorexia isn’t about weight - it’s about control, morality, and identity tied to “eating right”.
People with orthorexia:
Follow rigid “clean eating” rules
Avoid entire food groups (sugar, dairy, grains, oils, etc.)
Feel extreme guilt or shame after eating anything “impure”
May undergo frequent detoxes or cleanses
Lose weight unintentionally, but weight loss is not the primary goal
Proposed Diagnostic Criteria:
Criterion A: Obsessive focus on healthy eating, marked by:
Compulsive rules around what’s “good” and “bad” food
Emotional distress or shame when dietary rules are broken
Escalating restrictions over time (leading to weight loss or malnutrition)
Criterion B: These behaviors cause:
Physical complications (e.g., malnutrition, fatigue)
Social or academic disruptions (avoiding meals, events)
Self-worth becoming tied to adherence to the “clean” diet
The Emotional Cost:
Orthorexia is often praised in wellness spaces - but the person may be exhausted, isolated, and silently suffering. When “health” becomes punishment, something’s wrong.
In a world that glorifies clean eating, orthorexia hides in plain sight.
What Causes Eating Disorders?
There’s no single cause behind eating disorders - they emerge at the crossroads of biology, psychology, and culture. Often, what starts as a coping strategy slowly becomes a disorder. For many in India, it's not just about food or weight - it’s about control, fear, shame, and survival in a world that constantly comments on your body.
1. Biological Factors
Eating disorders have a strong genetic and neurobiological basis - they are not just a phase or a mindset.
A 2019 study found that anorexia nervosa shares genetic links with other mental health conditions like anxiety, depression, and OCD.
Behaviours like binge eating and vomiting have been found to be 46%–72% heritable.
First-degree relatives of those with anorexia or bulimia are 7 to 12 times more likely to have an eating disorder.
Brain chemicals like serotonin and dopamine - which regulate mood and reward - are often disrupted. This may contribute to binge eating, compulsive behaviors, and mood instability.
The gut-brain axis, still being studied, may also influence hunger signals, mood, and body image regulation.
Eating disorders are brain-based illnesses - not choices, not fads.
2. Psychological Factors
Certain personality traits and emotional patterns can increase vulnerability:
Perfectionism: A constant need to do things “right” - including eating, exercising, or looking a certain way.
Low self-esteem: Feeling “not enough” and using food or body control to gain a sense of worth.
History of trauma: Especially childhood abuse, bullying, or neglect.
Co-occurring disorders: Anxiety, depression, OCD, PTSD often exist alongside eating disorders.
3. Sociocultural Factors
In India, society's obsession with thinness, fairness, and control over women’s bodies often drives disordered patterns.
Bollywood & beauty filters reinforce unrealistic ideals of slimness and flawlessness.
Weight-focused parenting: Remarks like “don’t eat too much or you’ll get fat” are normalized.
Social media: Hashtags like #GlowUp and #WhatIEatInADay can quietly reinforce shame around natural bodies and appetites.
Marriage market pressure: Especially for women, there's an intense (often unspoken) need to appear “presentable” - slim, fair, and controlled.
Family policing: A girl who eats heartily or gains weight post-puberty is often seen as “undisciplined” or “problematic”.
Disordered eating isn’t always rebellion. Sometimes, it’s a desperate attempt to fit in, to be loved, to stay safe.
4. India-Specific Stressors
The cultural context here matters deeply.
Shame around normal body changes: Weight gain in PCOS, puberty, or pregnancy is treated like a flaw.
“Log kya kahenge” culture: The fear of judgment can push individuals to hide eating struggles - even from themselves.
Patriarchal norms: Strong women or those with bigger appetites may be mocked or judged - reinforcing the idea that a “controlled” woman is a “good” woman.
Signs & Symptoms: When to Seek Help
Eating disorders are not always visible. A person can seem “fine” while battling a war inside. Knowing the signs can help you or someone you love seek help early.
Emotional & Behavioral Signs
Obsession with food, weight, calories, or appearance
Avoiding meals or extreme meal-time anxiety
Secretive eating, hoarding, or hiding food
Feeling out of control around food
Using food to cope with emotions - bingeing, restricting, or purging
Distorted body image - never feeling “good enough”
Increased irritability, sadness, withdrawal, or mood swings
Physical Signs
Noticeable weight fluctuations (gain or loss)
Missed periods, low libido, or hormonal changes
Cold extremities, fatigue, dizziness, or fainting
Digestive issues, bloating, or food intolerance
Hair loss, dry skin, brittle nails
Brain fog and poor concentration
In Children:
Extreme pickiness that disrupts nutrition
Tantrums around meals
Sudden weight changes or refusal to eat entire food groups
Important: You don’t have to “look sick” to be struggling.
You don’t have to wait for things to get worse to seek support.
The Indian Silence: Why These Disorders Go Undiagnosed
In India, eating disorders often don’t look like what textbooks describe - and that’s exactly why they’re missed.
Despite growing awareness in urban spaces, the language, resources, and social permission to talk about disordered eating remain scarce.
1. No Words, No Language
In many Indian languages, there’s no direct translation for “eating disorder”. What might be anorexia is often brushed off as pet kam lagta hai (small appetite) or bimari ke baad kamzor ho gaya hai (she became weak after an illness).
Without the vocabulary, the suffering goes unnamed - and untreated.
2. Mistaken for “Discipline” or “Fasting”
Obsessive eating behaviours are frequently misread as virtues:
Skipping meals = good self-control
Avoiding carbs = fitness
Starving after festivals = cleansing
Culturally sanctioned practices like fasting during Navratri or Ramadan can sometimes overlap with disordered restriction - but intent matters. When control, fear, or guilt are the drivers, it’s no longer about faith or health.
3. Shame & Silence
Talking about food, body image, or mental health is still taboo in many households. For girls, expressing discomfort with body changes is often silenced with, “Sabko hota hai. Adjust karna padta hai”.
For boys, admitting to body dissatisfaction is often mocked: “Why do you care so much? Are you a model?”
The result? Shame becomes silence. Silence becomes suffering.
4. Gendered Expectations
Eating disorders affect all genders - but men are less likely to be diagnosed. Why? Because Indian masculinity often discourages emotional vulnerability and body talk.
Men with muscle dysmorphia or binge eating are more likely to be praised for their gym routines than to be seen as struggling.
5. Lack of Trained Professionals
In Tier 2 and Tier 3 cities, access to mental health professionals trained in eating disorders is rare. Even in metros, most therapists don’t receive specialised ED training, and medical professionals often miss the signs unless weight loss is extreme.
The danger is not just the disorder - it’s the silence that hides it.
Breaking that silence is the first step toward healing.
Long-Term Effects If Left Untreated
Eating disorders are not a phase. They are serious, progressive, and - without help - can lead to long-term harm across every system in the body.
1. Physical Health Consequences
Cardiovascular: Low heart rate, irregular heartbeat, heart failure
Reproductive: Missed periods, infertility, miscarriage risk
Skeletal: Bone thinning, early-onset osteoporosis
Gastrointestinal: Acid reflux, chronic constipation, damaged intestines
Endocrine: Hormonal imbalance, anemia, insulin resistance
Neurological: Poor concentration, memory issues, seizures
Electrolyte imbalances: Can lead to sudden cardiac arrest
Research shows that women who have struggled with eating disorders in the past often face long-term ripple effects. As adults, they are more likely to remain underweight, struggle with depression, smoke, or postpone childbirth. Many also experience complications during pregnancy - including severe nausea, unexplained bleeding, miscarriages, or even the need for medically induced abortions.
Another body of research links long-term undernourishment, especially in adolescents with anorexia, to lasting health issues such as stunted growth, fertility problems, and weakened bones due to early-onset osteoporosis.
2. Emotional & Social Impact
Suicidal thoughts & self-harm are common, especially in bulimia and anorexia
Strained friendships and family relationships
Disrupted education or career paths
Chronic low self-worth and emotional numbness
Isolation - not just from people, but from joy
3. Risk of Death
Eating disorders have a very high mortality rate among all mental health conditions - due to medical complications and suicide.
Getting help early can save a life - and restore one.
It’s never “too soon” or “not serious enough” to reach out.
Treatment That Heals Beyond Food
Eating disorders are not just about food - so recovery must reach far beyond the plate. True healing involves rewiring beliefs, emotions, and behaviors that have taken root over years. It’s about learning to live again, not just eat again.
Therapies That Work
1. CBT-E (Enhanced Cognitive Behavioral Therapy)
CBT-E is one of the most evidence-backed treatments for eating disorders across diagnoses. It helps people challenge distorted thoughts around food, weight, and self-worth, and establish regular, nourishing eating patterns.
The treatment typically progresses in four stages - as broken down by CBT-E Org:
Stage 1 focuses on understanding the eating problem and building structure around food.
Stage 2 is a brief review period to evaluate progress.
Stage 3 targets the root causes - like fear of weight gain, rigid rules, and emotional regulation.
Stage 4 prepares the person to maintain progress, prevent relapse, and move forward with life.
For underweight individuals, the process may include 40 sessions over 40 weeks, with a careful, collaborative approach to weight restoration.
2. DBT (Dialectical Behavior Therapy)
Originally developed for Borderline Personality Disorder (BPD), DBT is highly effective for eating disorders that involve emotional dysregulation - like bingeing or purging in response to distress.
A 12-month study showed that DBT significantly reduced both eating disorder and BPD symptoms, especially by improving coping skills. This approach teaches distress tolerance, emotion regulation, and interpersonal effectiveness - tools that many people with EDs never had the chance to build.
3. Family-Based Therapy (FBT)
FBT empowers caregivers - especially in adolescents - to take an active role in refeeding and recovery. It’s not about blame; it’s about building a support system that the eating disorder can’t thrive in.
FBT has shown strong success in treating anorexia and bulimia in children and teens, and is increasingly adapted for ARFID and atypical presentations as well.
4. Schema Therapy
For individuals who carry deep-rooted beliefs like “I am only lovable if I’m thin” or “I must be in control to be safe”, schema therapy can be life-changing. It targets these long-standing patterns and helps people rebuild a more compassionate relationship with themselves.
5. Psychoanalytic Therapy
While slower-paced, this approach is helpful for those whose eating disorders are closely tied to trauma, early attachment issues, or identity conflicts. It allows space to explore not just behavior, but the unconscious pain underneath it.
6. Nutrition Counseling
With the help of a trained dietitian who understands eating disorders, individuals learn to rebuild trust in hunger cues, challenge food fears, and create a balanced relationship with eating. It’s not about dieting - it’s about nourishing body and mind.
7. Medication
While not a standalone treatment, medications may help manage co-occurring conditions like depression, anxiety, or OCD - which often coexist with eating disorders and can make recovery harder without support.
Prevention & Healing at Home: Building Food Peace Early
Eating disorders often begin quietly - in subtle restrictions, anxious meal times, or offhand comments about weight. But with mindful habits and language, homes can become places of prevention, not pressure.
Whether you or your loved ones are struggling, or simply want to foster a healthier environment, here are everyday tools that nourish both body and mind:
Practice Mindful Eating
Eat slowly, without screens. Learn to listen to your body’s cues - hunger, fullness, satisfaction - instead of rushing through meals or ignoring discomfort.Body Neutrality Over Body Judgment
Shift from asking “Do I look good?” to “How do I feel today?” Appreciate your body for what it can do - digest, dance, carry you through life - not just how it looks.Challenge Diet Talk
Replace “good food vs bad food” with “all foods fit”. Labeling foods morally often creates guilt and shame that fuel disordered eating.Support Regular Meals
Predictable eating patterns help stabilize energy, emotions, and appetite. It’s not about being rigid - it’s about offering safety through rhythm.Celebrate Cultural Foods Without Guilt
Indian food traditions are inherently nurturing. Whether it’s khichdi for gut comfort, curd for cooling, or ghee for strength - there’s healing in heritage.Move for Joy, Not Punishment
Redefine movement: a morning walk, dancing to your favorite song, stretching at night. Let it feel like care, not compensation.Foster Open Conversations
Don’t wait for a crisis. Create non-judgmental spaces where body image, mental health, and identity can be spoken about - and heard with care.
Urging a Loved One to Seek Help (With Compassion)
When someone you care about is struggling, it’s natural to feel helpless or unsure of what to say. But the right words, tone, and timing can plant seeds for healing.
Don’t blame or accuse.
Instead of “Why are you doing this to yourself?” try:
“I’ve noticed you seem really anxious around food lately. I’m here if you ever want to talk.”Offer support, not solutions.
Try: “Would you like me to help you look for someone to talk to?” or “We can figure this out together.”Avoid comments on appearance.
Even praise like “You look healthier now!” can be misunderstood. Focus on how they feel, not how they look.Be patient.
Denial is common - not from deceit, but from fear or shame. Keep showing up without pressure.Encourage professional help.
Healing requires trained support - not just willpower or home remedies.
Recovery Is Not Linear
It’s filled with steps forward and steps back. But what matters is showing up again, and again. You don’t have to be “sick enough” to deserve help. You just have to begin.
How Are Eating Disorders Diagnosed?
Many people don’t recognize they’re struggling - or they hide it out of fear. But early diagnosis can prevent years of suffering and even save lives.
Step 1: Consult a Doctor or Mental Health Professional
Start by speaking with someone you trust - a therapist, psychiatrist, or even a primary care doctor.
Step 2: Medical Assessments
These help rule out physical complications and nutritional deficiencies:
Weight and height monitoring
Vital signs: blood pressure, heart rate
Blood and urine tests to evaluate electrolytes, hormones, liver and kidney function
Step 3: Psychological Evaluations
Clinical interviews exploring food behaviors, beliefs, and emotional history
Self-report tools like the Eating Disorder Examination Questionnaire (EDE-Q) or SCOFF
Assessment of co-occurring issues like anxiety, depression, trauma, or OCD
An official diagnosis is typically made using DSM-5-TR criteria, but even without a label, the need for care is valid. If food and body thoughts are interfering with daily life - help is not only allowed, it’s essential.
Spotlight: Hidden Eating Disorders in Indian Culture
Eating disorders in India don’t always scream for attention. They whisper - through rituals of discipline, wellness, and control.
The bride who fasts obsessively before her wedding, so she can “look perfect” in photos - even if it means fainting during fittings.
The gym bro who spirals into panic if he misses a workout, afraid his “gains” will disappear overnight.
The diabetic teen who eats painfully “clean”, not out of health, but fear - of judgment, stigma, and being seen as undisciplined.
The working mother who skips meals just to feel a shred of control in her chaotic day - praised as “strong” but silently starving.
The young woman who avoids eating out with friends to stay “pure” on her diet - believing one slip ruins everything.
These stories don’t always come with a diagnosis. They don’t always look like illness.
But they carry the same pain - and they deserve the same care.
How Elfina Can Help
At Elfina, we understand that eating disorders are more than food or weight. They’re woven into emotions, identity, family roles, and cultural pressures.
That’s why our care is holistic, empathetic, and culturally attuned:
🎓 Trained Experts: Work with licensed therapists who specialize in eating disorders, body image, and co-occurring mental health concerns like anxiety, trauma, or OCD.
🪞 Contextual Therapy: Our therapists understand the Indian context - fatphobia, “log kya kahenge”, generational body shame, and perfectionism.
🧠 Integrated Support: Our team includes both mental health professionals and nutrition specialists - because healing isn’t just mental or physical. It’s both.
🤝 At Your Pace: Whether you're ready for deep work or just starting to explore your relationship with food, Elfina meets you where you are - with compassion, not pressure.
🔒 Confidential & Accessible: 100% online, confidential, and available no matter your location or stage of struggle.
🌟 94% of clients are matched with a suitable therapist on the first try.
🌟 80%+ of our therapists have 5+ years of clinical experience.
Whether you’re surviving in silence, supporting a loved one, or just wondering if something is off - you are not alone.
Elfina is here to walk with you toward food freedom, self-trust, and emotional healing.
Frequently Asked Questions (FAQs)
Can you recover from an eating disorder without therapy?
Some people make progress through self-help, supportive communities, or personal insight - but for most, therapy is essential. Eating disorders are deeply rooted in thoughts, emotions, and behaviors. A trained therapist can help unpack the “why” behind disordered patterns and support long-term healing.
Do men have eating disorders?
Absolutely. While underdiagnosed, eating disorders affect people of all genders. Muscle dysmorphia, compulsive exercise, and binge eating often show up differently in men - and may be overlooked due to stigma or cultural expectations around masculinity.
Is fasting for religious reasons considered disordered eating?
Not necessarily. But it can become disordered when religious fasting is used to mask restriction or control weight.
A study in the Journal of Eating Disorders found that religious participants who altered their eating for both spiritual and weight-control reasons experienced greater disordered eating and appearance-related pressure than those who didn’t change their diet.
What if I don’t feel “sick enough”?
There is no such thing as not being “sick enough” to deserve help.
Eating disorders are mental illnesses, not defined by appearance or weight. If your thoughts, habits, or emotions around food cause distress - you deserve care.
How do I talk to my child if I suspect they have an eating disorder?
Start with gentle concern, not confrontation. Try:
“I’ve noticed some changes and I care about how you’re feeling - can we talk about it?”
Avoid comments about appearance. Instead, focus on emotions, stress, or behaviors. Consider reaching out to a therapist for support - for them, and for you.
Conclusion: Food Is Not the Enemy. Shame Is.
Eating disorders are not vanity.
They are not weakness.
They are not something you can simply “snap out of”.
They are often a quiet cry for control, connection, and peace - disguised as food rules, skipped meals, or relentless self-criticism.
You are not “too much”.
You are not “too dramatic”.
You are not “too far gone”.
You deserve joy. Nourishment. A relationship with food that feels safe - not punishing.
At Elfina, we believe recovery is not about perfection. It’s about coming home to yourself.
Whether you’re noticing the first signs or have lived with this struggle for years - it’s not too late. It’s not too mild. And it’s definitely not your fault.
Elfina’s therapists and nutrition specialists are here to walk with you - with empathy, cultural understanding, and clinical care.
Healing is possible. You don’t have to do it alone.
Other blogs

Frequently Asked Questions
What types of therapy do you offer?
Can I meet my therapist in-person?
How do you match me with a therapist?
How much does therapy cost?
Do you offer free trials?
Finding The Right Fit, Made Easy





© Mindaro Health Technologies. All rights reserved
© Mindaro Health Technologies. All rights reserved
Finding the right fit, made easy.
FAQs
What types of therapy do you offer?
Can I meet my therapist in-person?
How do you match me with a therapist?
How much does therapy cost?
Do you offer free trials?