What Are Personality Disorders? A Complete Guide to Symptoms, Causes & Treatment
|
15
min read
|
Tanvi

Introduction
Not every difficult personality is a disorder. But when certain ways of thinking, feeling, and behaving become rigid, distressing, and hard to change - they may be signs of a personality disorder.
According to the American Psychiatric Association, personality disorders involve “pervasive patterns of perceiving, relating to, and thinking about the environment and the self that interfere with long-term functioning”. These patterns aren't just quirks - they cause deep distress or disrupt daily life, work, and relationships.
These disorders often begin in adolescence or early adulthood, continuing for years without proper support or understanding.
But let’s take a step back.
We all have personality traits - like being cautious, emotional, outgoing, or detail-oriented. These traits exist on a spectrum, and most people show a healthy mix of them depending on the situation. For example, someone might be highly agreeable at work, but more assertive at home.
However, when a personality trait becomes extreme, inflexible, and harmful - and affects nearly every area of life - it might fall into the realm of a personality disorder.
This blog is here to untangle the complexity with clarity and compassion - because people with personality disorders deserve help, not harsh labels.
What Are Personality Disorders?
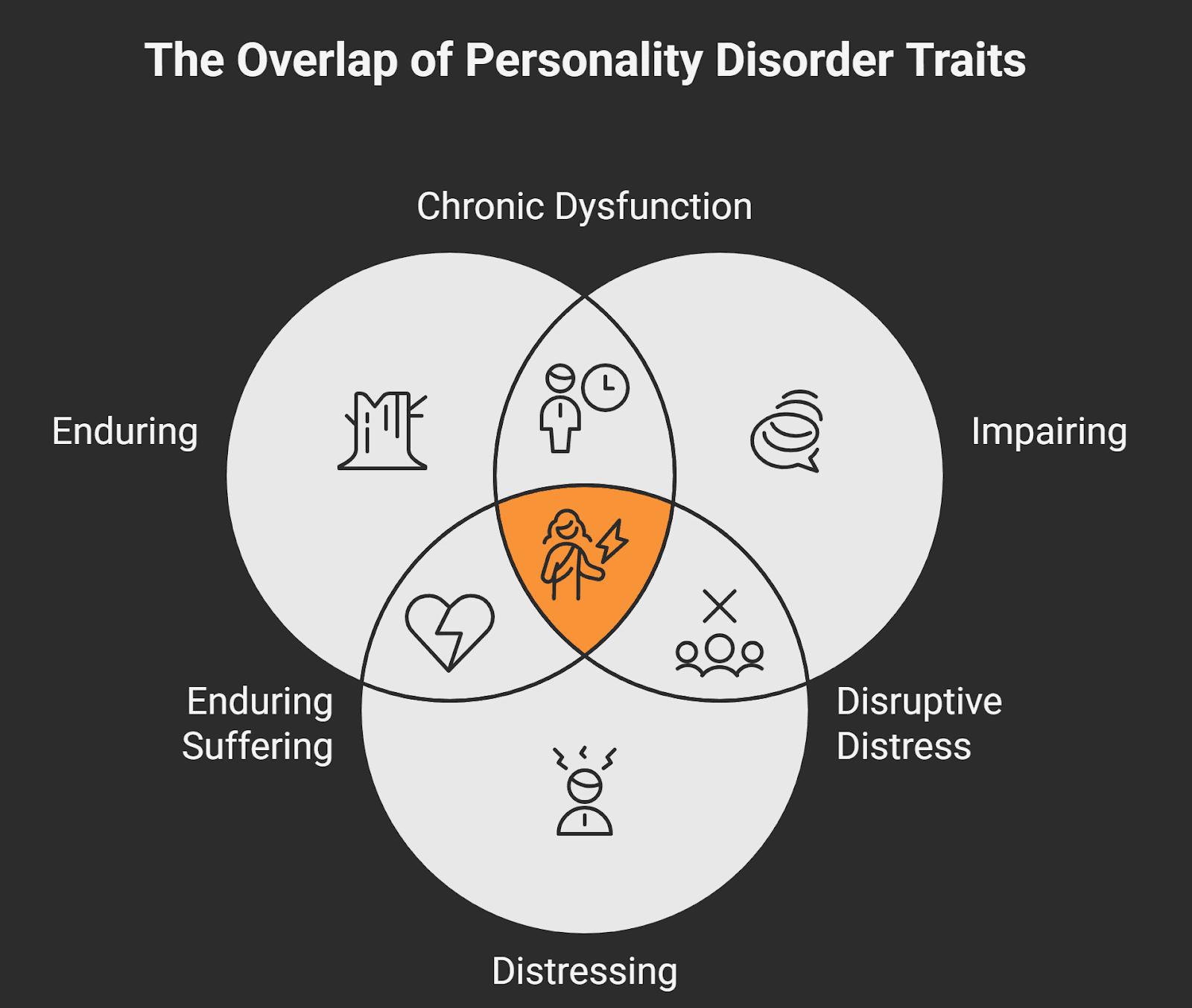
At their core, personality disorders are:
Enduring: They last for years, often a lifetime without treatment.
Impairing: They interfere with jobs, friendships, family dynamics, and even identity.
Distressing: Both for the person experiencing it and for those around them.
They involve long-term patterns of behavior, emotion, and thinking that differ significantly from cultural expectations. These patterns can affect:
How someone sees themselves and others
How they manage emotions
How they respond to stress or conflict
How they form and maintain relationships
Most personality disorders begin to show signs in adolescence or early adulthood. And according to research, nearly 9.1% of the general population lives with one.
Importantly, these are not simply "bad habits" or "attitude problems". They reflect deep, inner experiences - often rooted in early trauma, temperament, or chronic invalidation.
Per the DSM-5, for a diagnosis of personality disorder, the pattern must be:
"Enduring, inflexible, and pervasive across a broad range of personal and social situations...and must lead to clinically significant distress or impairment."
Many individuals with personality disorders also struggle with co-occurring issues like anxiety, depression, eating disorders, or substance use, which can make diagnosis and recovery more complex - but not impossible.
📜 A Brief History of Personality Disorder Classification
Long before modern psychology, humans were trying to make sense of the mind.
Around 400 BCE, Hippocrates described four core “temperaments” based on bodily fluids - sanguine (optimistic), choleric (irritable), melancholic (sad), and phlegmatic (calm). He linked these patterns to both physical and emotional traits, noting how environmental factors like climate could influence emotional states. While not scientific by today’s standards, it was an early attempt to understand personality patterns.
Fast-forward to the 20th century, the DSM-I (1952) first introduced “personality disturbances” - broad categories that attempted to capture maladaptive traits.
As research progressed, psychiatry shifted from psychoanalytic interpretations to more evidence-based frameworks. The current DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition) recognizes 10 specific personality disorders, grouped into three clusters:
Cluster A (Odd/Eccentric): Paranoid, Schizoid, Schizotypal
Cluster B (Dramatic/Emotional): Antisocial, Borderline, Histrionic, Narcissistic
Cluster C (Anxious/Fearful): Avoidant, Dependent, Obsessive-Compulsive
Each cluster shares common characteristics - but individuals may show traits across different clusters, and diagnoses can overlap or evolve over time.
Understanding these categories isn’t about labeling - it’s about offering clarity, empathy, and paths to healing.
The Three Clusters of Personality Disorders

According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), personality disorders are grouped into three clusters based on descriptive similarities. Each disorder within these clusters reflects enduring and pervasive patterns of behavior, cognition, and inner experience that deviate markedly from cultural expectations and significantly impair functioning.
Let’s start with Cluster A, which is often misunderstood and underdiagnosed.
Cluster A: Odd or Eccentric Disorders
These disorders are characterized by social withdrawal, distorted thinking, and behaviors that others may perceive as unusual or strange. People in this cluster often struggle with forming close relationships - not because they don’t want to, but because they experience fundamental challenges in trust, perception, or emotional connection. Psych Central notes that emotional unavailability may also be a sign of cluster A
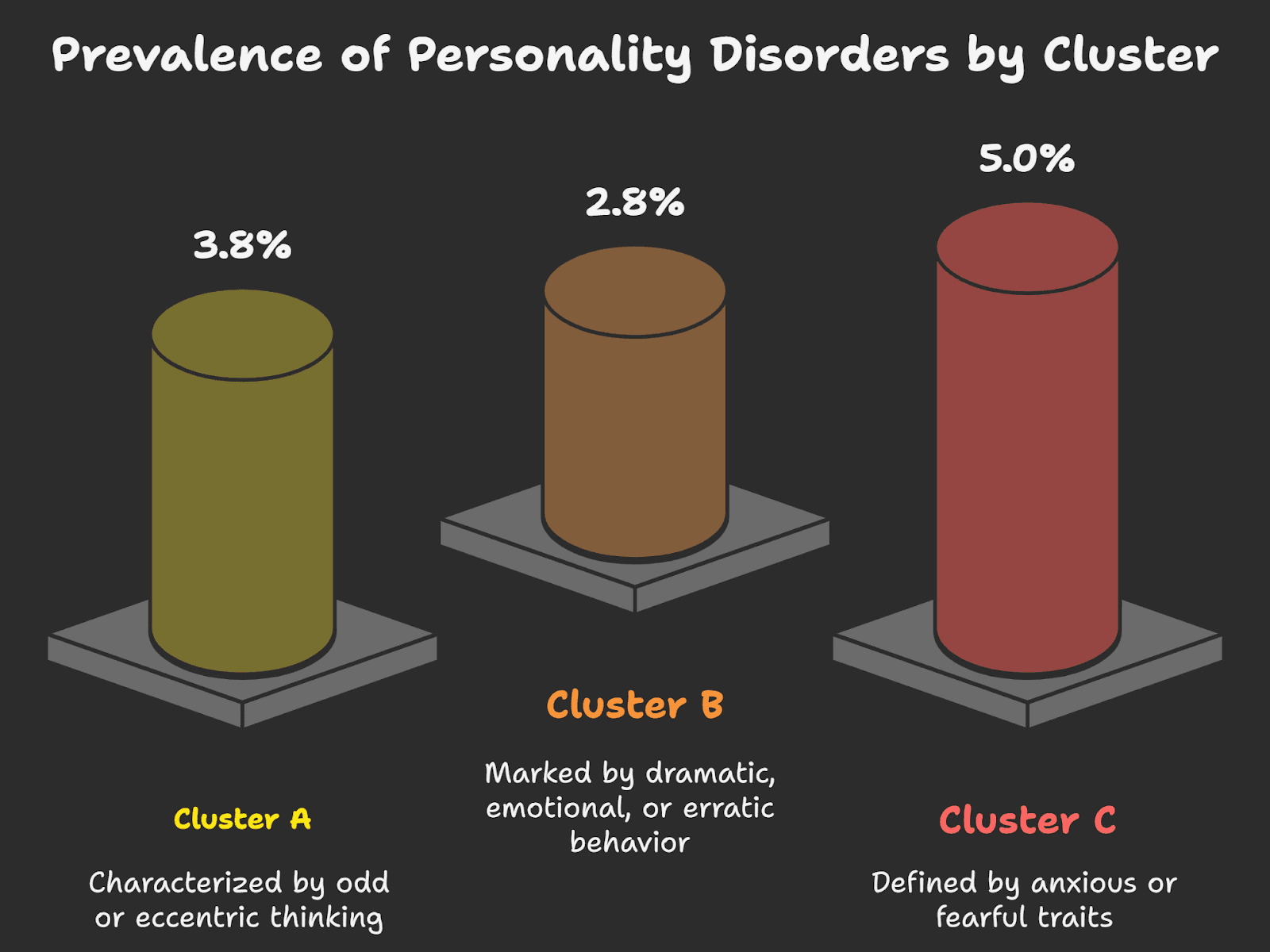
📊 Globally, about 3.8% of people are estimated to live with a Cluster A personality disorder.
1. Paranoid Personality Disorder (PPD)
Marked by deep mistrust and suspicion of others - even when there's no apparent reason to be distrustful.
DSM-5-TR Diagnostic Criteria (4 or more symptoms):
Constant suspicion that others have hidden agendas or intend to harm you
Frequent doubts about the loyalty or honesty of friends or coworkers
Hesitant to open up due to fear the information will be turned against you
Overinterpreting neutral comments or events as threatening
Holding grudges or being unable to forgive perceived slights
Believing others are constantly attacking your character, and often reacting angrily
Unfounded doubts that your romantic partner is being faithful
🎬 Howard Hughes in The Aviator – portrayed by Leonardo DiCaprio – shows classic PPD features: extreme distrust, isolation, and obsession with control.
🧠 Insight: PPD may be more prevalent among those with family histories of schizophrenia or delusional disorder. Trauma or maltreatment in early childhood can also be contributing factors.
🛑 Treatment Challenge: Healthline mentions how Individuals with PPD often mistrust therapists themselves, making treatment engagement difficult.
2. Schizoid Personality Disorder (SPD)

Defined by emotional detachment, limited expression, and a strong preference for solitude. These individuals aren’t just introverted - they often feel little to no desire for close relationships.
DSM-5-TR Diagnostic Criteria (4 or more symptoms):
Lack of desire for close relationships, including with family
Strong preference for being alone in most activities
Little interest in sexual experiences with others
Rarely finds joy in most life activities
Has no close confidants beyond immediate family
Seems emotionally distant or detached
Appears unaffected by praise or criticism from others
Tyler J. Torrico et al. highlight how those with SPD are often described as emotionally blunted, aloof, and disengaged.
Origin Insight: The disorder tends to emerge in early adulthood and is often a defense mechanism rooted in insecure attachment or emotional neglect.
3. Schizotypal Personality Disorder (STPD)

This disorder lies at the intersection of personality dysfunction and psychotic-like symptoms. It’s characterized by eccentric behaviors, social anxiety, and cognitive or perceptual distortions.
Psychology Today indicates that the speech of individuals with this condition may feature digressions, unusual word choices, or signs of magical thinking, including beliefs in clairvoyance and bizarre fantasies. Patients typically experience distorted thought processes and shy away from intimacy.
DSM-5-TR Diagnostic Criteria (5 or more symptoms):
Believes unrelated events have personal meaning (ideas of reference)
Holds magical or superstitious beliefs that affect actions
Perceives the world in unusual or distorted ways
Often suspicious or believes others have harmful intent
Has peculiar speech patterns or abstract language
Suffers from ongoing social anxiety, even with familiar people
Has limited or flat emotional expression
Exhibits eccentric mannerisms or an unusual appearance
Has few or no close relationships outside immediate family
🪄 Luna Lovegood in Harry Potter - though not a pathological example - illustrates the eccentric thinking and social awkwardness often seen in schizotypal individuals.
📚 Research Insight: Raine (2006) suggests two types of STPD - one more biological (linked to schizophrenia spectrum) and one more psychosocial (based on early emotional adversity and inconsistent attachment).
🧬 Men may be at slightly higher risk for schizotypal traits than women.
🧠 Summary: Cluster A in Context
Disorder | Key Feature | Diagnostic Highlights (DSM-5) | Character Illustration |
Paranoid PD | Mistrust & suspicion | Reads hidden motives, avoids confiding, holds grudges | Howard Hughes (The Aviator) |
Schizoid PD | Emotional detachment | Prefers solitude, emotionally cold, indifferent to feedback | - |
Schizotypal PD | Eccentric thoughts | Magical thinking, odd speech, high social anxiety | Luna Lovegood (Harry Potter) |
While these disorders may resemble psychotic disorders on the surface, they do not involve full-blown delusions or hallucinations. That’s why accurate diagnosis using DSM-5 criteria is critical.
Cluster B: Dramatic, Emotional, or Erratic Disorders
These disorders are marked by intense emotional expression, impulsivity, difficulty regulating feelings, and unpredictable interpersonal behavior. People with Cluster B disorders often struggle to maintain stable relationships, not out of malice, but due to deep-rooted emotional dysregulation and identity confusion.
📊 An estimated 2.8% of the global population lives with a Cluster B personality disorder.
Healthline & DSM-5-TR Note: To be diagnosed with a Cluster B personality disorder:
Symptoms must begin by early adulthood.
If diagnosed before age 18, symptoms must be present for at least one year.
Symptoms should not be attributable to another mental disorder, substance use, or acute stressor.
1. Borderline Personality Disorder (BPD)
Marked by emotional instability, intense relationships, and a deep fear of abandonment. BPD is often misunderstood as “moodiness”, but it goes far deeper - rooted in chronic pain, identity confusion, and attachment trauma.
DSM-5-TR Diagnostic Criteria: (5 or more symptoms)
Desperate efforts to avoid real or imagined abandonment
Unstable, intense relationships swinging between idealization and devaluation
Identity confusion or unstable self-image
Impulsivity in potentially harmful areas (e.g., sex, substance use, reckless spending)
Recurrent suicidal thoughts or self-harming behaviors
Intense emotional reactivity and mood shifts
Chronic feelings of emptiness
Inappropriate or uncontrollable anger
Temporary stress-related paranoia or dissociation
💡 Clinical Insight:
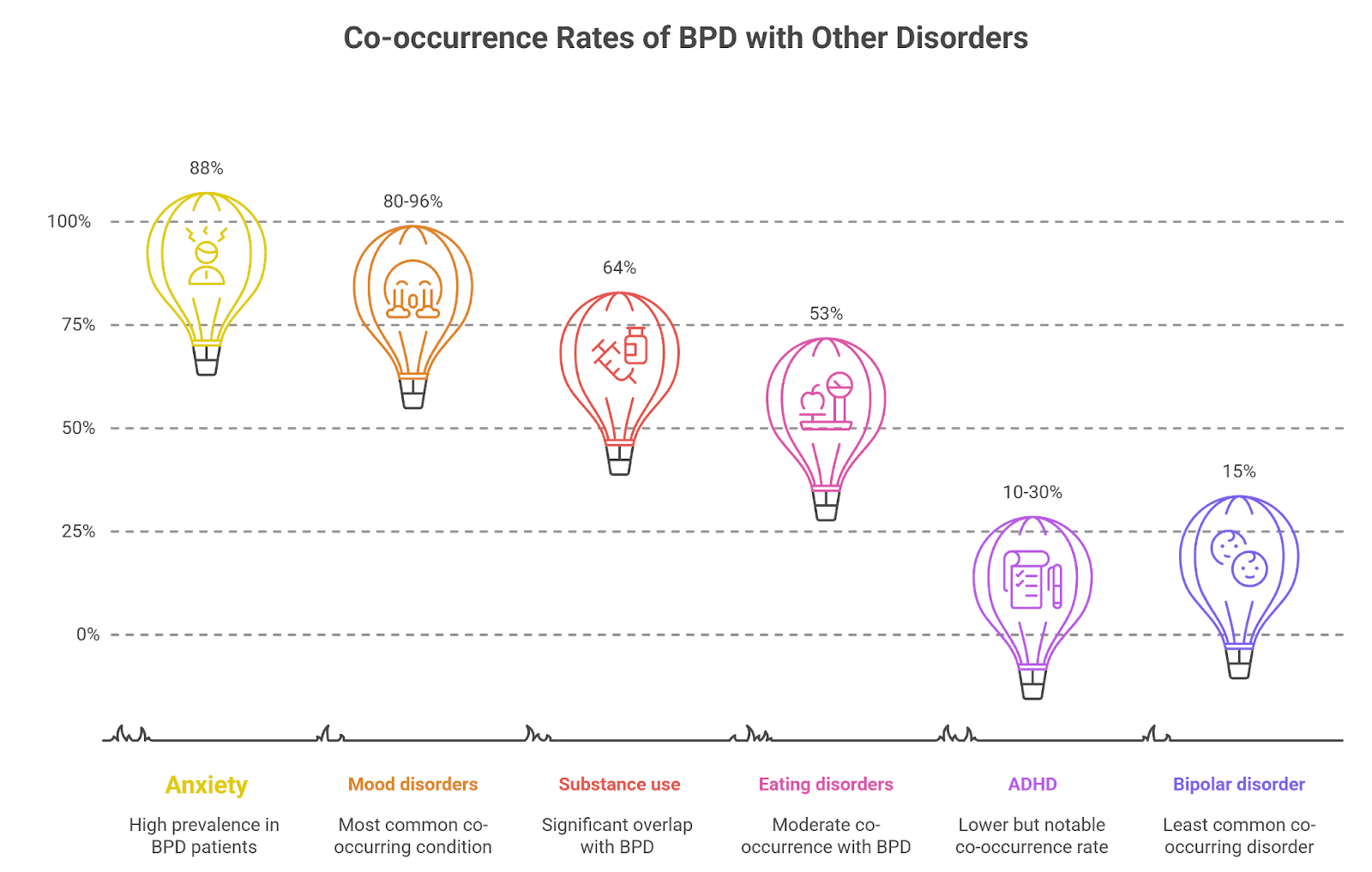
Cleveland Clinic reports BPD often co-occurs with:
Mood disorders (80–96%)
Anxiety (88%)
Substance use (64%)
Eating disorders (53%)
ADHD (10–30%)
Bipolar disorder (15%)
🧬 Risk Factors (as per Mayo Clinic):
Genetic vulnerability
Emotional neglect or abuse in early childhood
Unstable attachments with caregivers
🛠️ Treatment Note: Dialectical Behavior Therapy (DBT) has transformed outcomes for many with BPD, helping develop emotional regulation, distress tolerance, and interpersonal skills.
2. Antisocial Personality Disorder (ASPD)
Defined by a pervasive disregard for others’ rights, manipulation, and lack of remorse. It’s not just “being mean” - it involves chronic patterns of deceit, aggression, and impulsive rule-breaking.
DSM-5-TR Diagnostic Criteria: (3 or more symptoms)
Repeated law-breaking or criminal behavior
Chronic dishonesty or use of aliases for personal gain
Impulsive decision-making or poor planning
Frequent aggression or involvement in fights
Reckless disregard for personal or others’ safety
Irresponsibility in work or financial obligations
Lack of guilt or rationalizing mistreatment of others
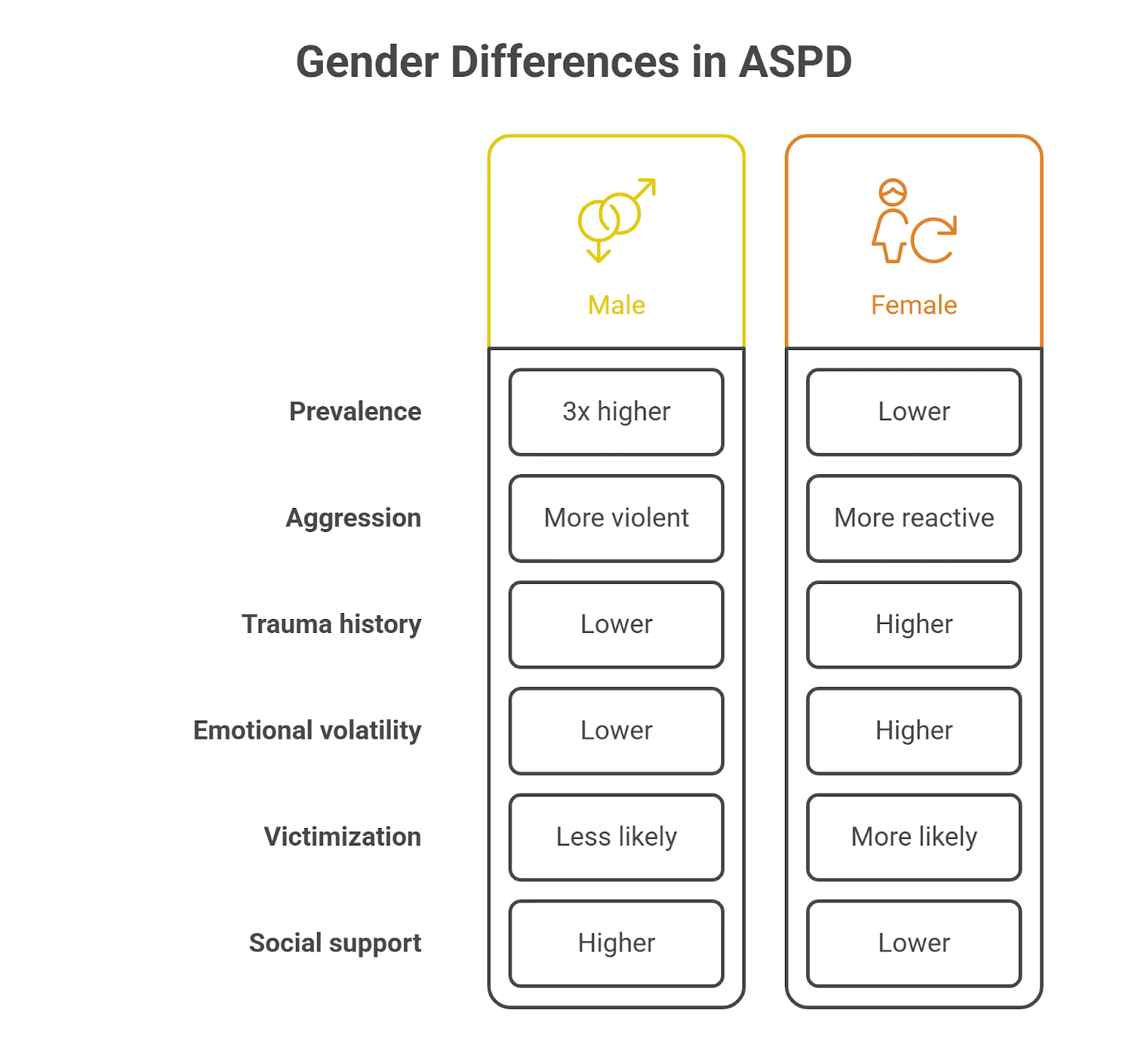
🔎 Gender Differences:
Research shows a 3:1 male-to-female ratio, though women with ASPD may present more emotional volatility and higher trauma histories. According to research, they often have less violent but more reactive aggression and are more likely to experience victimization and lack of support.
🧠 Clinical Challenge: People with ASPD rarely seek therapy voluntarily, and often present with charm that masks deeper patterns of manipulation.
Therapists actively engage with patients, families, and interdisciplinary teams to discuss the diagnosis, anticipated course, and management plans for antisocial personality disorder.
3. Histrionic Personality Disorder (HPD)

HPD is characterized by excessive emotionality and attention-seeking. Individuals with this disorder are often perceived as dramatic or flirtatious, but these behaviors are unconscious attempts to gain connenction and reassurance.
DSM-5-TR Diagnostic Criteria: (5 or more symptoms)
Discomfort when not the center of attention
Inappropriate flirtatious or seductive behavior
Rapidly shifting and shallow emotional expressions
Constant use of appearance to gain attention
Style of speech that lacks detail or is impressionistic
Dramatic or exaggerated emotional displays
High suggestibility or easily influenced by others
Misjudging the closeness of relationships
🧬 Comorbidities: Frequently overlaps with narcissistic, borderline, and antisocial traits. HPD is not about manipulation - these behaviors often arise from deep fears of being ignored or unseen.
🧠 Social Insight: Individuals may act theatrically in professional or inappropriate settings without awareness of how it’s perceived.
4. Narcissistic Personality Disorder (NPD)
NPD involves patterns of inflated self-importance, fragile self-esteem, and a constant need for validation. It’s not just arrogance - it’s often a deep vulnerability masked by grandiosity or manipulation.
Treating Narcissistic Personality Disorder is often challenging. Individuals with NPD commonly hold grandiose fantasies and are convinced they deserve special treatment. These characteristics typically emerge by early adulthood and must be consistently evident across various contexts, including professional and personal relationships.
DSM-5-TR Diagnostic Criteria: (5 or more symptoms)
Grandiose view of self and exaggerated achievements
Fantasies of unlimited power, beauty, or success
Belief in being uniquely special or only understood by high-status individuals
Need for excessive admiration
Sense of entitlement or expecting special treatment
Manipulating others for personal gain
Lack of empathy
Envious of others or belief that others envy them
Arrogant, haughty behaviors or attitudes
🧠 Harvard Health notes NPD is 50–75% more common in males, and is associated with elevated risk of depression, social conflict, and even suicide.
🎬 Fictional Illustration: Walter White from Breaking Bad embodies both covert and overt narcissism - swinging between self-righteous justification and emotional cruelty.
💬 Insight: NPD can be covert (insecure, hypersensitive) or overt (dominant, grandiose). Often, people with NPD avoid therapy or present with a “false self” that hides vulnerability.
🧠 Summary: Cluster B in Context
Disorder | Key Feature | DSM-5-TR Criteria Highlights | Character Illustration |
Borderline PD | Instability in mood, identity, and relationships | Fear of abandonment, impulsivity, emotional swings | – |
Antisocial PD | Disregard for rights of others | Lawbreaking, deceit, aggression, lack of remorse | – |
Histrionic PD | Emotionality and attention-seeking | Needs to be center of attention, dramatic behavior | – |
Narcissistic PD | Grandiosity and fragile self-esteem | Entitlement, lack of empathy, need for admiration | Walter White (Breaking Bad) |
⚠️ Reminder: Cluster B traits can be extremely painful for those living with them. They often stem from unresolved emotional wounds, early trauma, or learned survival mechanisms. Accurate diagnosis using DSM-5-TR criteria and trauma-informed therapy can change lives.
Cluster C: Anxious or Fearful Disorders
Cluster C personality disorders are defined by persistent patterns of fear, anxiety, and behavioral avoidance. These individuals often crave connection, stability, or control - but their inner fears can hold them back from relationships, growth, and emotional freedom.
According to mentalhealth.com, a struggle to interact correctly with others and to advance in life often leads individuals with this condition to exist on the fringes of society.
📊 Globally, about 5.0% of the population lives with a Cluster C personality disorder - the highest prevalence among all three clusters.
🧠 DSM-5-TR Note: These traits must be:
Long-standing (starting in early adulthood)
Rigid across personal and professional contexts
Causing significant distress or functional impairment
Not better explained by another mental health condition
1. Avoidant Personality Disorder (AVPD)

Marked by deep feelings of inadequacy, extreme fear of criticism, and chronic social withdrawal - despite a strong desire for closeness. This isn’t just shyness; it’s an inner voice that constantly whispers “you’re not good enough”.
Females could have a somewhat elevated chance of developing the condition.
🧠 DSM-5-TR Diagnostic Criteria (4 or more symptoms):
Avoids social jobs or activities out of fear of criticism or rejection
Withholds from personal connections unless certain of being liked
Holds back in close relationships due to fear of ridicule
Worries obsessively about disapproval or rejection in public spaces
Reluctant to try new social situations out of fear of not being good enough
Sees self as socially inept, inferior, or unappealing
Avoids risks or new ventures that could lead to embarrassment
🧠 Emotional Insight:
While AVPD often appears as “quiet” or “withdrawn”, many individuals yearn for relationships - they’re just afraid they’ll never be accepted.
📚 Origins: Childhood environments with excessive criticism, shame, or conditional affection can increase risk. Parenting styles that emphasized guilt, perfection, or emotional distance are frequently reported.
🎬 Fictional Illustration: Neville Longbottom in Harry Potter exemplifies AVPD traits - timid, self-doubting, and fearful of criticism, yet deeply loyal and capable when given time and trust.
2. Dependent Personality Disorder (DPD)
DPD is characterized by an overwhelming need to be cared for, leading to submissive behaviors and fear of abandonment. People with DPD often feel incapable of making decisions without others’ input.
🧠 DSM-5-TR Diagnostic Criteria (5 or more symptoms):
Needs constant advice or reassurance for everyday decisions
Requires others to take responsibility for major life areas
Fears expressing disagreement in relationships
Avoids initiating tasks due to lack of self-confidence
Will go to uncomfortable lengths to receive support or care
Feels helpless or panicked when alone due to fear of being unable to cope
Desperately seeks another relationship after one ends
Overwhelming fear of being abandoned or left alone
🧠 Behavioral Insight: These individuals aren’t manipulative - they are deeply afraid of abandonment and often feel incapable of standing alone.
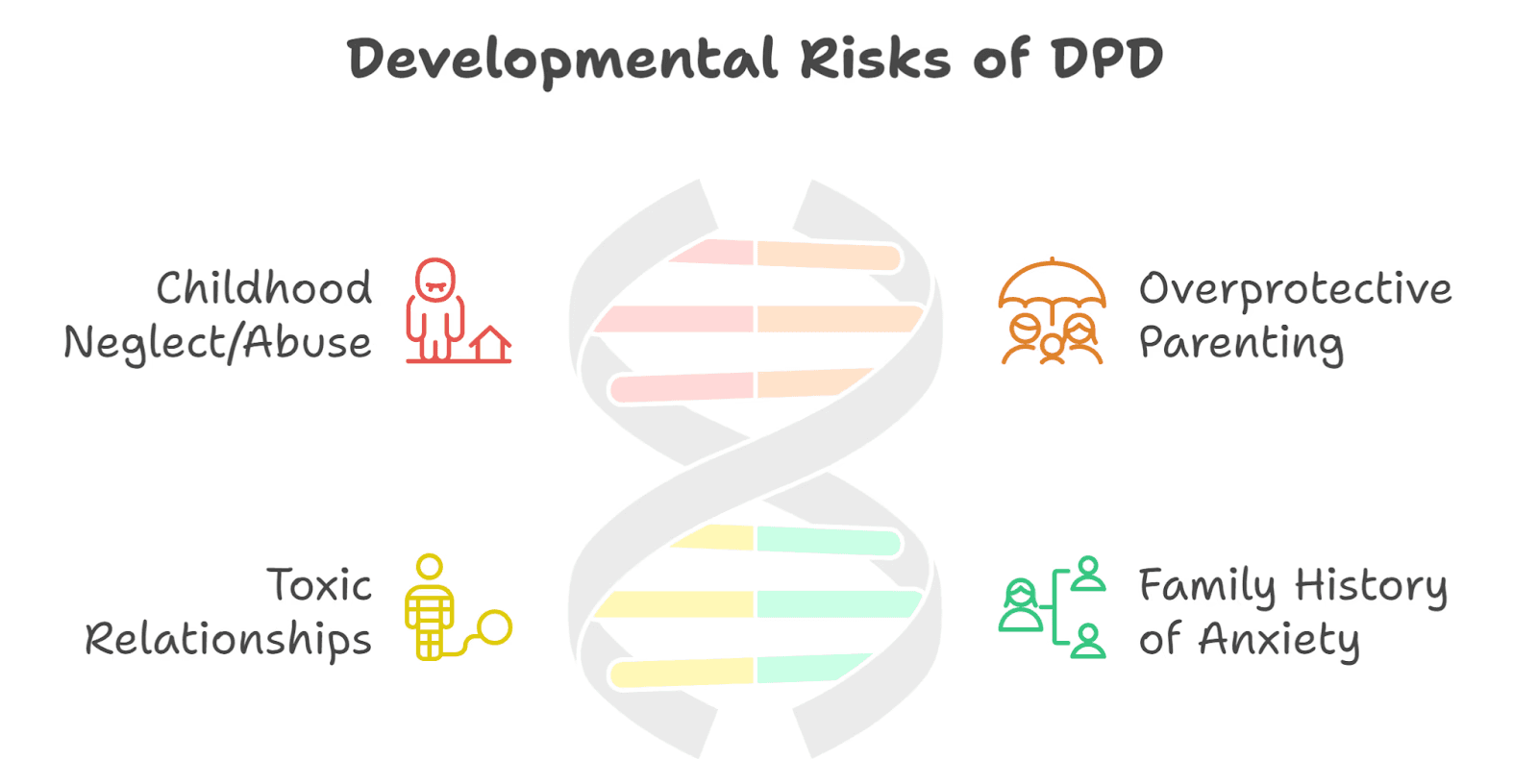
📚 Developmental Risks (as per Healthline):
Neglect or abuse in childhood
Overprotective, authoritarian parenting
Long-term toxic or controlling relationships
Family history of anxiety disorders
💬 DPD rarely presents with impulsivity or anger; instead, it often hides behind soft-spokenness, people-pleasing, and fear of disappointing others.
3. Obsessive-Compulsive Personality Disorder (OCPD)

OCPD is not the same as OCD. While OCD is marked by intrusive thoughts and rituals, OCPD is a personality style focused on perfectionism, control, and moral rigidity. People with OCPD often pride themselves on their discipline - but may not recognize how it negatively impacts others.
🧠 DSM-5-TR Diagnostic Criteria (4 or more symptoms):
Preoccupied with rules, details, order, or schedules - even if it ruins the bigger purpose
Perfectionism that blocks task completion
Excessive devotion to work and productivity, ignoring recreation and relationships
Overly rigid or morally inflexible values
Inability to discard old or useless possessions
Hesitates to delegate tasks unless others follow their exact methods
Miserly approach to spending - saves excessively for potential disaster
Displays stubbornness and rigidity in beliefs or routines
🧠 Clinical Difference:
Unlike OCD, individuals with OCPD often do not see their behavior as problematic. They may believe their way is the “right way” and feel frustrated when others don’t live up to their standards.
📚 OCD UK notes: People with OCPD often have little insight into their behavior, while those with OCD usually recognize their thoughts as irrational and seek help.
🎬 Fictional Illustration: Sheldon Cooper in The Big Bang Theory represents OCPD traits - strict routines, intense perfectionism, and low tolerance for deviation, often creating friction in relationships.
🧠 Summary: Cluster C in Context
Disorder | Key Feature | DSM-5-TR Criteria Highlights | Character Illustration |
Avoidant PD | Fear of rejection and inadequacy | Avoids risks, social anxiety, extreme self-criticism | Neville Longbottom (Harry Potter) |
Dependent PD | Excessive need for care | Cannot make decisions alone, fears abandonment | – |
Obsessive-Compulsive PD | Perfectionism and control | Rigid, overly rule-bound, controlling of self and others | Sheldon Cooper (Big Bang Theory) |
⚠️ Reminder: Cluster C disorders are often mistaken for anxiety or introversion. But these patterns are more pervasive, emotionally consuming, and impair daily functioning.
Therapy can help reframe beliefs, increase self-worth, and build healthier relationships.
Spotlight on Narcissistic Personality Disorder (NPD)
Narcissistic Personality Disorder (NPD) is one of the most misunderstood mental health conditions. It’s often associated with arrogance, entitlement, and vanity - but beneath that surface, it can mask a fragile and deeply wounded sense of self.
People with NPD often struggle with chronic feelings of inadequacy, even if they appear confident or successful. Their need for admiration, control, or validation may be rooted in early emotional injuries, shame, or unmet attachment needs.
Overt vs. Covert Narcissism
NPD isn’t always loud.
Overt narcissism is easier to spot - it involves grandiosity, dominance, and visible entitlement.
Covert narcissism, however, is quieter and harder to detect. These individuals may appear sensitive, shy, or anxious, but underneath lies hypersensitivity to rejection, deep envy, and a need for constant reassurance.
Both types can involve intense emotional reactions - including narcissistic rage - when their ego is wounded. This might look like explosive anger, passive-aggressive behavior, or long periods of withdrawal and stonewalling.
In close relationships, this can lead to a painful cycle:
Idealization (love-bombing or putting you on a pedestal)
Devaluation (emotional withdrawal, criticism, or control)
Discard (pulling away or blaming you)
...and then it starts again.
People who live with or care for someone with NPD often describe feeling like they’re walking on eggshells - unsure when the next outburst might come or whether the affection they’re receiving is real.
What Makes NPD Difficult to Spot
Because people with NPD can be charismatic, articulate, or highly successful, they’re often overlooked in clinical settings. Their distress might be masked by charm or defensiveness, making it harder for therapists or even close family members to recognize what’s going on beneath the surface.
That’s why therapy can be especially complex. There’s currently no standardized, manualized therapy for NPD, but Mentalization-Based Treatment (MBT) offers a promising approach. It helps individuals reflect on their internal emotional states and understand how their behavior impacts others - without shame or blame.
The “SPECIAL ME” Framework
Duke Health recommends this acronym to understand the diagnostic picture:
Sense of self-importance
Preoccupied with power, success, or beauty
Entitled
Can only associate with “special” people
Interpersonally exploitative
Arrogant behavior
Lack of empathy
Must be admired constantly
Envious of others (or believes others envy them)
NPD is not about selfishness. It’s about identity, attachment, and fear. And with the right support, healing is possible - even if it’s hard-earned.
Spotlight: Borderline Personality Disorder (BPD)
Borderline Personality Disorder is often reduced to “intense emotions” or “mood swings”, but that framing misses the deeper truth. At its core, BPD is a condition shaped by deep emotional sensitivity, a longing for connection, and an overwhelming fear of abandonment.
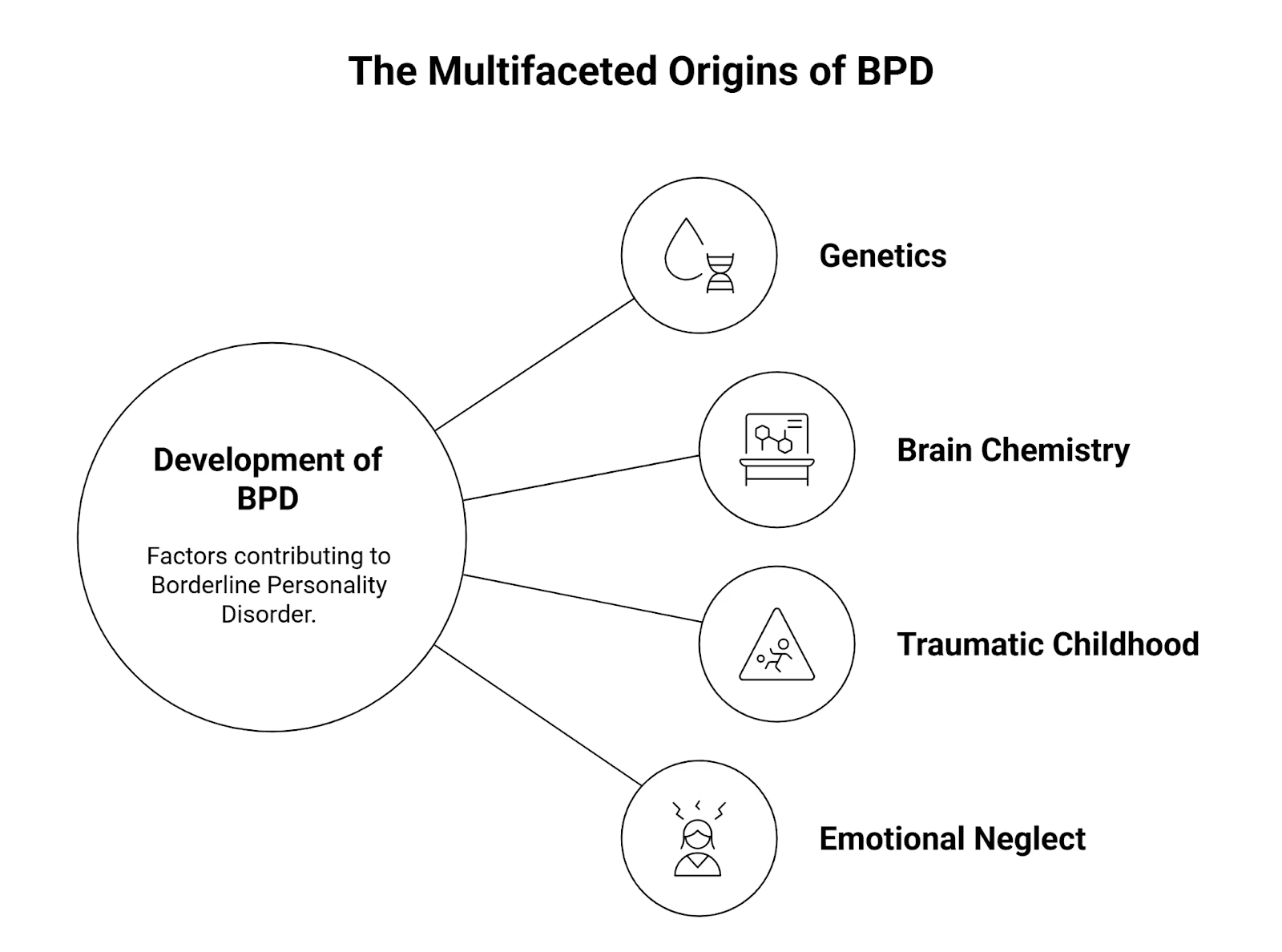
Psychology Today suggests a few reasons why someone might develop BPD. It often comes down to a mix of things like your genetics, the chemical makeup of your brain, and tough experiences growing up. This could mean a traumatic childhood with abusive or unpredictable parents. Plus, severe emotional neglect as a child also plays a big part.
People with BPD often feel emotions more acutely than others. Love, rejection, sadness, anger - it all hits harder and lasts longer. When someone they care about pulls away, even briefly, the fear of abandonment can be so intense that it feels unbearable. And in trying to avoid that abandonment, they may act impulsively - even in ways they regret later.
The Pain Behind the Behavior
What’s often seen as “dramatic” or “unstable” is actually a survival strategy. Many individuals with BPD have lived through emotional neglect, trauma, or chaotic caregiving. Their nervous systems were never taught how to trust, regulate, or feel safe in relationships.
This shows up as:
Splitting - seeing people & situations as all good or all bad, shifting rapidly between idealization and disappointment. Splitting can sometimes be done as a defence mechanism.
Impulsivity - reacting without a filter when overwhelmed by emotions
Chronic emptiness - feeling like they don’t know who they really are without external validation
It’s important to note: many people with BPD are deeply empathetic and loving. But the pain of being left - or the idea that they might be - can lead them to push others away before they themselves are pushed.
A Life-Changing Treatment: DBT
Dialectical Behavior Therapy (DBT) has brought tremendous hope for people with BPD. It combines mindfulness with emotion regulation, distress tolerance, and interpersonal effectiveness.
We’ll explore DBT in more detail later, but for now, know this: BPD is not untreatable. With the right therapeutic environment, many people go on to lead grounded, fulfilling, and emotionally rich lives.
How Do You Know If Someone Has a Personality Disorder?
One of the most important - and confusing - aspects of personality disorders is that they’re not always obvious. Many people with personality disorders function well in certain areas of life. They may be high-achieving at work or socially charismatic, but still struggle deeply with relationships, self-worth, or emotional control.
It’s About Patterns, Not Moments
A diagnosis isn’t based on isolated incidents. It’s based on long-standing patterns that show up across settings - in work, friendships, family, or romantic relationships.
According to PsychCentral, two or more of the following areas are usually impacted:
How a person thinks about themselves and others (cognitions)
Emotional range and stability (affect)
Interpersonal relationships
Impulse control
If these issues cause chronic distress or disruption, especially when they’ve been present since adolescence or early adulthood, a personality disorder may be part of the picture.
For Parents and Caregivers
In young people, early signs may include:
Persistent black-and-white thinking (“everyone hates me” vs. “everyone loves me”)
Intense fear of rejection
Ongoing conflicts in friendships
Difficulty managing anger or impulse-driven behavior
But remember - diagnosis is not about labeling. It’s about understanding. And that understanding can only come through a careful clinical process involving:
Structured interviews (like the SCID-5)
Psychological tools (like the Personality Inventory for DSM-5 or PID-5)
A clear history of behavior patterns over time
If someone you love seems to be struggling, compassion - not confrontation - is the first step. Personality disorders don’t define someone’s worth. But naming the problem can be the beginning of healing.
What Causes Personality Disorders?

Personality disorders don’t come out of nowhere. They often develop from a complex mix of genetics, early environment, temperament, and social experiences - all of which shape how we learn to relate to the world and to ourselves.
The American Psychological Association (APA) outlines several contributing factors with key research references:
1. Genetic Predisposition
While there’s no single “personality disorder gene”, research suggests that genetics can influence the development of traits like fear, anxiety, aggression, and emotional sensitivity - which may, in turn, increase vulnerability to personality disorders.
For example, one research team identified a malfunctioning gene linked to obsessive-compulsive traits, while others have explored genetic links to impulsivity and emotional dysregulation, key features in many disorders.
2. Childhood Trauma and Emotional Environment
The Collaborative Longitudinal Personality Disorders Study found a strong connection between childhood trauma and later personality dysfunction.
Borderline personality disorder, in particular, was strongly linked to early experiences of sexual trauma.
Even verbal abuse, such as being frequently yelled at or emotionally rejected by caregivers, was shown to increase the risk of developing borderline, narcissistic, obsessive-compulsive, or paranoid traits in adulthood.
These early experiences disrupt a child’s ability to form secure attachments and to regulate their emotions - key building blocks of personality development.
3. Temperament and Reactivity
Some children are more emotionally sensitive or reactive than others. Known as high reactivity, this temperament makes them more easily overwhelmed by stress, change, or sensory input - which can affect how they relate to others.
According to APA, this kind of biological sensitivity may increase the likelihood of developing shy, withdrawn, or anxious personality styles, especially if paired with an invalidating or unpredictable environment.
4. Protective Social Factors
Not all children exposed to adversity develop personality disorders. The APA notes that positive relationships - with a caregiver, teacher, or even a single friend - can offset negative influences and build emotional resilience.
Addition: Neurobiology and Brain Structure
Structural and functional differences in the brain are also implicated.
Neuroimaging studies have identified abnormalities in areas related to emotion regulation, impulse control, and social cognition, especially in people with borderline personality disorder (BPD):
Reduced gray matter in regions like the amygdala, hippocampus, ventral cingulate gyrus, and orbitofrontal cortex
Differences based on sex: BPD women tend to show reduced volume in the medial temporal lobe, while BPD men show more changes in the anterior cingulate cortex
These changes aren’t the sole cause of personality disorders, but they may amplify emotional sensitivity, impulsivity, and relational difficulties - especially when combined with environmental stress.
How Personality Disorders Affect Life
Personality disorders are often invisible from the outside - but for the person living with one, the impact touches nearly every part of daily life. From relationships to self-worth, the effects are chronic, deep-rooted, and emotionally exhausting.
1. Relationships
Many people with personality disorders want close, stable relationships - but may find themselves stuck in patterns of:
Fear of abandonment or rejection
Overdependence or emotional detachment
Explosive conflict or emotional withdrawal
What starts as love or connection can quickly spiral into mistrust, insecurity, or misunderstanding.
2. Work and Career
At work, challenges may include:
Difficulty accepting feedback or criticism
Struggles with authority, rigid rules, or collaboration
Emotional dysregulation that leads to burnout, frequent job changes, or underperformance
Even highly capable individuals may self-sabotage or feel chronically “not good enough”.
3. Self-Image and Identity
Living with a personality disorder can feel like never really knowing who you are. Common issues include:
Shame, self-hatred, or deep-seated feelings of inadequacy
Difficulty maintaining a stable sense of self
Constant self-doubt and fear of how others perceive you
4. Mental Health Struggles
Personality disorders often co-occur with other mental health conditions like:
Depression
Anxiety
Substance use
Eating disorders
PTSD or trauma-related disorders
Without integrated care, these conditions can intensify each other, making recovery harder.
5. Suicide Risk
Because of the intense emotional pain and impulsivity involved, people with certain personality disorders - particularly borderline personality disorder - are at higher risk for self-harm and suicide.
This makes early recognition, compassion, and professional intervention all the more critical.
Substance Use and Co-Occurring Disorders
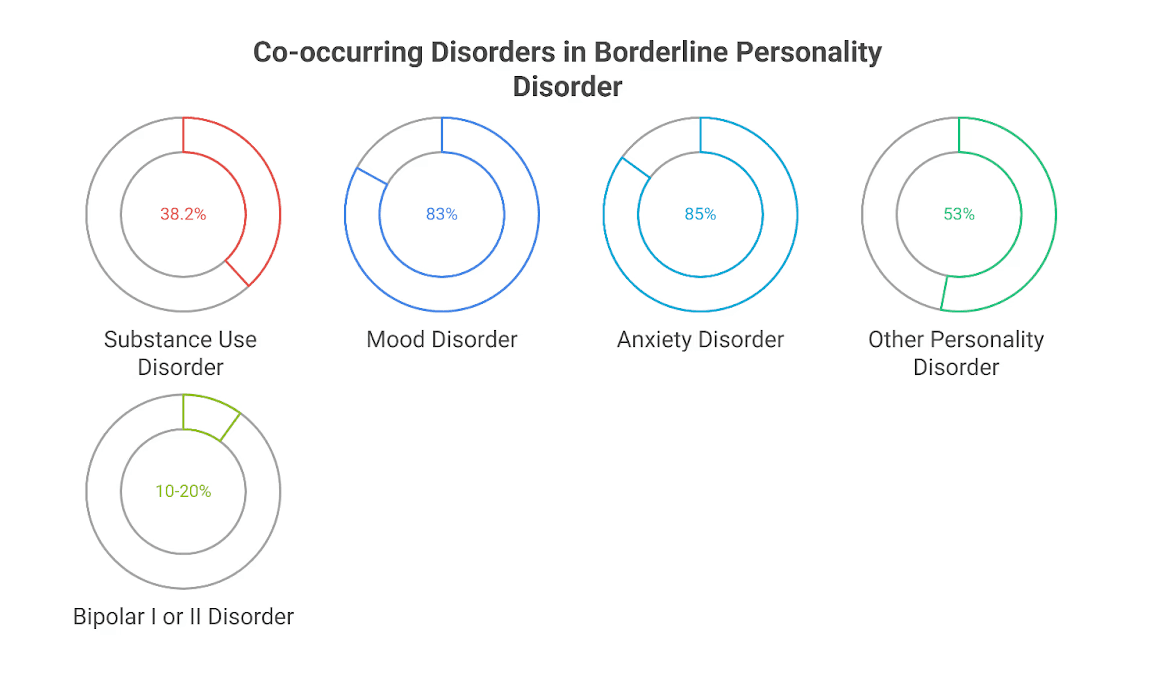
Personality disorders rarely show up in isolation. Most individuals experience co-occurring disorders, especially when it comes to substance use.
According to the US National Institute of Mental Health (NIMH):
Around 22.6% of people with any personality disorder also have a substance use disorder (SUD)
Among those with BPD, this rate jumps to 38.2%
Other studies report:
83% of individuals with BPD have a mood disorder
85% have an anxiety disorder
53% meet criteria for another personality disorder
10–20% have bipolar I or II disorder
Why Does This Happen?
For many, substances like alcohol, cannabis, or stimulants become a way to manage emotional pain, numb feelings of emptiness, or feel “in control”.
However, substance use can worsen emotional regulation, increase impulsivity, and make therapy less effective - leading to a cycle that’s hard to break.
People with Cluster B disorders, in particular, face an increased risk of suicidal ideation, which becomes even more dangerous when substance use is involved.
If Left Untreated
When personality disorders go unrecognized or untreated, the long-term impact can be profound. These are not just “difficult personalities” - they’re mental health conditions that shape every aspect of life.
1. Chronic Emotional Pain
Without treatment, many individuals experience:
Lifelong patterns of distress, emptiness, or rage
Repeated feelings of failure or unworthiness
Cycles of conflict, isolation, and disconnection
2. Risk of Harm
Untreated personality disorders are linked to:
Higher rates of self-harm
Increased suicide attempts
More frequent use of substances to cope
3. Relationship and Parenting Difficulties
Struggles with emotional regulation and trust can make it hard to:
Parent consistently or set healthy boundaries
Maintain long-term partnerships
Build mutual respect in relationships
4. Stalled Personal Growth
Many individuals find it difficult to:
Stay in school or hold down jobs
Trust therapists or stick with treatment
Set and achieve long-term goals
But none of this is inevitable. With compassionate care and the right therapeutic approach, personality disorders can be treated - and people can lead meaningful, connected, and fulfilling lives.
Treatment That Works
Personality disorders aren’t character flaws - they’re deeply rooted patterns of thinking, feeling, and relating that often begin in childhood and become harder to shift over time. That’s why treatment is possible, but it takes time, patience, and the right support system.
Therapy is the cornerstone. Medications may help with specific symptoms, but meaningful change typically happens in the context of a stable therapeutic relationship, where emotional patterns can be gently understood and transformed.
Dialectical Behavior Therapy (DBT): Especially Effective for BPD
Originally developed for borderline personality disorder, DBT has become one of the most evidence-based treatments for helping people manage emotional intensity, self-destructive behaviors, and relationship struggles.
What sets DBT apart is its balance between acceptance and change. It doesn’t just teach you how to stop destructive behaviors - it helps you understand where they come from.
DBT helps build four essential skills:
Mindfulness: Being present without judgment
Distress Tolerance: Surviving crisis moments without making things worse
Emotion Regulation: Naming, understanding, and managing big feelings
Interpersonal Effectiveness: Learning to ask for what you need while maintaining self-respect and relationships
People with BPD often describe DBT as life-changing. For many, it’s the first time they learn how to sit with overwhelming emotions - instead of being ruled by them.
CBT, Schema, and Psychodynamic Therapies
While DBT is a great fit for BPD, other therapies are helpful for different personality disorders:
Cognitive Behavioral Therapy (CBT) focuses on reframing distorted thinking patterns and building healthier behaviors.
Schema Therapy blends CBT with emotional healing. It explores how early unmet needs can create lifelong “schemas” - like feeling unlovable or defective - and helps individuals rewrite those narratives.
Psychoanalytic or Psychodynamic Therapy looks at unconscious patterns and how early relationships shaped the self. These longer-term approaches can help people gain deep insight into why they relate the way they do - and begin to do it differently.
Medication: Helpful, But Not a Cure
According to Mind UK, there are no medications specifically designed for personality disorders. However, doctors may prescribe:
Antidepressants (for persistent sadness or hopelessness)
Mood stabilizers (for intense mood swings or irritability)
Antipsychotics (for paranoia or severe disorganization)
These are usually prescribed for co-occurring conditions like depression or anxiety, rather than the core personality traits themselves.
Support During Life Transitions
People with personality disorders often need additional support during major life transitions, such as:
Pregnancy and parenting
Grief or relationship endings
Job loss or retirement
Moving out of the family home
These changes can unearth old fears or destabilize coping strategies. Therapy during these periods isn’t just helpful - it can be essential for maintaining progress and emotional safety.
Can Personality Disorders Be Prevented?
We often think of personality disorders as something that “just happens” in adulthood - but the roots are almost always laid down early. That’s why early prevention, especially emotional attunement in childhood, can make a lasting difference.
“Borderline personality disorder may be the most preventable of all mental illnesses.”
- Interpreted from Dr. Andrew Chanen’s work, 2013
While most prevention research has focused on BPD, the principles apply broadly: supportive environments, secure attachments, and emotional literacy reduce risk - and help children grow into emotionally resilient adults.
What Helps?
1. Emotionally Attuned Caregiving
Children who feel seen, soothed, and supported are more likely to develop a stable sense of self and trust in others.
They learn that:
Feelings are valid
Mistakes don’t mean rejection
Relationships can survive conflict
This kind of caregiving helps prevent the shame, fear, and identity confusion often seen in personality disorders later in life.
2. Secure Attachment and Role Models
Caregivers who model healthy emotional expression - naming their feelings, calming themselves, repairing conflict - give children a roadmap for handling their own emotions and relationships.
Even one safe adult, whether a parent, teacher, or relative, can become a buffer against early trauma or neglect.
3. Emotionally Healthy School and Community Environments
Prevention also goes beyond the home. Schools that teach emotional intelligence, empathy, and communication skills can give children the tools to navigate conflict, set boundaries, and handle rejection - key protective factors.
Communities that reduce stigma and promote access to early mental health care can also help identify and address problems before they solidify into personality patterns.
A Final Word on Prevention
Not every personality disorder can be prevented. Genetics, temperament, and life experiences all play a role. But creating emotionally nurturing environments - at home, in school, and in society - can significantly lower risk.
And for those already struggling: it’s never too late to heal. Prevention matters. But so does compassion, support, and therapy at any age.
How Elfina Can Help
At Elfina, we believe that therapy should feel like being truly seen - not judged.
Living with a personality disorder can often mean carrying years of pain, shame, or confusion. Many people feel misunderstood, dismissed, or afraid to reach out. That’s why we’ve built a therapy experience that prioritizes trust, cultural sensitivity, and deep emotional safety.
Here’s what makes Elfina different:
🎯 94% therapist-client match on the very first try
Because healing starts with the right person.👩⚕️ 80%+ of our therapists have 5+ years of experience
We work with specialists who understand complex trauma, personality patterns, and the emotional depth behind the diagnosis.🧘 Culturally aware and trauma-informed care
Our therapists understand the unique emotional landscapes shaped by family, culture, and societal expectations - especially in South Asian and Indian contexts.🔒 Judgment-free, confidential spaces for long-term healing
Whether you're struggling with identity, fear of abandonment, emotional regulation, or just trying to understand why relationships feel so difficult - you don’t have to face it alone.
At Elfina, we don’t rush you. We meet you where you are, at your pace, with compassion and clinical care. Because therapy isn’t just about managing symptoms - it’s about rebuilding your relationship with yourself.
Conclusion: This Is Not the End - It’s a Beginning
A personality disorder is not a brokenness.
It’s not a failure of character.
And it’s certainly not something to be ashamed of.
It’s a way of describing deeply persistent emotional patterns — ones that were often shaped by early wounds, unmet needs, or survival strategies that no longer serve us.
But with therapy, support, and self-compassion, these patterns can change.
People with personality disorders can and do:
Build stable, loving relationships
Create meaningful careers
Learn to feel safe in their own emotions
Reconnect with joy, purpose, and peace
It’s not easy. Healing takes time. But it is absolutely possible.
At Elfina, we’re honored to walk that path with you - step by step, with the respect and care you deserve. 💙


What Are Personality Disorders? A Complete Guide to Symptoms, Causes & Treatment
|
15
min read
|
Tanvi
Introduction
Not every difficult personality is a disorder. But when certain ways of thinking, feeling, and behaving become rigid, distressing, and hard to change - they may be signs of a personality disorder.
According to the American Psychiatric Association, personality disorders involve “pervasive patterns of perceiving, relating to, and thinking about the environment and the self that interfere with long-term functioning”. These patterns aren't just quirks - they cause deep distress or disrupt daily life, work, and relationships.
These disorders often begin in adolescence or early adulthood, continuing for years without proper support or understanding.
But let’s take a step back.
We all have personality traits - like being cautious, emotional, outgoing, or detail-oriented. These traits exist on a spectrum, and most people show a healthy mix of them depending on the situation. For example, someone might be highly agreeable at work, but more assertive at home.
However, when a personality trait becomes extreme, inflexible, and harmful - and affects nearly every area of life - it might fall into the realm of a personality disorder.
This blog is here to untangle the complexity with clarity and compassion - because people with personality disorders deserve help, not harsh labels.
What Are Personality Disorders?
At their core, personality disorders are:
Enduring: They last for years, often a lifetime without treatment.
Impairing: They interfere with jobs, friendships, family dynamics, and even identity.
Distressing: Both for the person experiencing it and for those around them.
They involve long-term patterns of behavior, emotion, and thinking that differ significantly from cultural expectations. These patterns can affect:
How someone sees themselves and others
How they manage emotions
How they respond to stress or conflict
How they form and maintain relationships
Most personality disorders begin to show signs in adolescence or early adulthood. And according to research, nearly 9.1% of the general population lives with one.
Importantly, these are not simply "bad habits" or "attitude problems". They reflect deep, inner experiences - often rooted in early trauma, temperament, or chronic invalidation.
Per the DSM-5, for a diagnosis of personality disorder, the pattern must be:
"Enduring, inflexible, and pervasive across a broad range of personal and social situations...and must lead to clinically significant distress or impairment."
Many individuals with personality disorders also struggle with co-occurring issues like anxiety, depression, eating disorders, or substance use, which can make diagnosis and recovery more complex - but not impossible.
📜 A Brief History of Personality Disorder Classification
Long before modern psychology, humans were trying to make sense of the mind.
Around 400 BCE, Hippocrates described four core “temperaments” based on bodily fluids - sanguine (optimistic), choleric (irritable), melancholic (sad), and phlegmatic (calm). He linked these patterns to both physical and emotional traits, noting how environmental factors like climate could influence emotional states. While not scientific by today’s standards, it was an early attempt to understand personality patterns.
Fast-forward to the 20th century, the DSM-I (1952) first introduced “personality disturbances” - broad categories that attempted to capture maladaptive traits.
As research progressed, psychiatry shifted from psychoanalytic interpretations to more evidence-based frameworks. The current DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition) recognizes 10 specific personality disorders, grouped into three clusters:
Cluster A (Odd/Eccentric): Paranoid, Schizoid, Schizotypal
Cluster B (Dramatic/Emotional): Antisocial, Borderline, Histrionic, Narcissistic
Cluster C (Anxious/Fearful): Avoidant, Dependent, Obsessive-Compulsive
Each cluster shares common characteristics - but individuals may show traits across different clusters, and diagnoses can overlap or evolve over time.
Understanding these categories isn’t about labeling - it’s about offering clarity, empathy, and paths to healing.
The Three Clusters of Personality Disorders
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), personality disorders are grouped into three clusters based on descriptive similarities. Each disorder within these clusters reflects enduring and pervasive patterns of behavior, cognition, and inner experience that deviate markedly from cultural expectations and significantly impair functioning.
Let’s start with Cluster A, which is often misunderstood and underdiagnosed.
Cluster A: Odd or Eccentric Disorders
These disorders are characterized by social withdrawal, distorted thinking, and behaviors that others may perceive as unusual or strange. People in this cluster often struggle with forming close relationships - not because they don’t want to, but because they experience fundamental challenges in trust, perception, or emotional connection. Psych Central notes that emotional unavailability may also be a sign of cluster A
📊 Globally, about 3.8% of people are estimated to live with a Cluster A personality disorder.
1. Paranoid Personality Disorder (PPD)
Marked by deep mistrust and suspicion of others - even when there's no apparent reason to be distrustful.
DSM-5-TR Diagnostic Criteria (4 or more symptoms):
Constant suspicion that others have hidden agendas or intend to harm you
Frequent doubts about the loyalty or honesty of friends or coworkers
Hesitant to open up due to fear the information will be turned against you
Overinterpreting neutral comments or events as threatening
Holding grudges or being unable to forgive perceived slights
Believing others are constantly attacking your character, and often reacting angrily
Unfounded doubts that your romantic partner is being faithful
🎬 Howard Hughes in The Aviator – portrayed by Leonardo DiCaprio – shows classic PPD features: extreme distrust, isolation, and obsession with control.
🧠 Insight: PPD may be more prevalent among those with family histories of schizophrenia or delusional disorder. Trauma or maltreatment in early childhood can also be contributing factors.
🛑 Treatment Challenge: Healthline mentions how Individuals with PPD often mistrust therapists themselves, making treatment engagement difficult.
2. Schizoid Personality Disorder (SPD)
Defined by emotional detachment, limited expression, and a strong preference for solitude. These individuals aren’t just introverted - they often feel little to no desire for close relationships.
DSM-5-TR Diagnostic Criteria (4 or more symptoms):
Lack of desire for close relationships, including with family
Strong preference for being alone in most activities
Little interest in sexual experiences with others
Rarely finds joy in most life activities
Has no close confidants beyond immediate family
Seems emotionally distant or detached
Appears unaffected by praise or criticism from others
Tyler J. Torrico et al. highlight how those with SPD are often described as emotionally blunted, aloof, and disengaged.
Origin Insight: The disorder tends to emerge in early adulthood and is often a defense mechanism rooted in insecure attachment or emotional neglect.
3. Schizotypal Personality Disorder (STPD)
This disorder lies at the intersection of personality dysfunction and psychotic-like symptoms. It’s characterized by eccentric behaviors, social anxiety, and cognitive or perceptual distortions.
Psychology Today indicates that the speech of individuals with this condition may feature digressions, unusual word choices, or signs of magical thinking, including beliefs in clairvoyance and bizarre fantasies. Patients typically experience distorted thought processes and shy away from intimacy.
DSM-5-TR Diagnostic Criteria (5 or more symptoms):
Believes unrelated events have personal meaning (ideas of reference)
Holds magical or superstitious beliefs that affect actions
Perceives the world in unusual or distorted ways
Often suspicious or believes others have harmful intent
Has peculiar speech patterns or abstract language
Suffers from ongoing social anxiety, even with familiar people
Has limited or flat emotional expression
Exhibits eccentric mannerisms or an unusual appearance
Has few or no close relationships outside immediate family
🪄 Luna Lovegood in Harry Potter - though not a pathological example - illustrates the eccentric thinking and social awkwardness often seen in schizotypal individuals.
📚 Research Insight: Raine (2006) suggests two types of STPD - one more biological (linked to schizophrenia spectrum) and one more psychosocial (based on early emotional adversity and inconsistent attachment).
🧬 Men may be at slightly higher risk for schizotypal traits than women.
🧠 Summary: Cluster A in Context
Disorder | Key Feature | Diagnostic Highlights (DSM-5) | Character Illustration |
Paranoid PD | Mistrust & suspicion | Reads hidden motives, avoids confiding, holds grudges | Howard Hughes (The Aviator) |
Schizoid PD | Emotional detachment | Prefers solitude, emotionally cold, indifferent to feedback | - |
Schizotypal PD | Eccentric thoughts | Magical thinking, odd speech, high social anxiety | Luna Lovegood (Harry Potter) |
While these disorders may resemble psychotic disorders on the surface, they do not involve full-blown delusions or hallucinations. That’s why accurate diagnosis using DSM-5 criteria is critical.
Cluster B: Dramatic, Emotional, or Erratic Disorders
These disorders are marked by intense emotional expression, impulsivity, difficulty regulating feelings, and unpredictable interpersonal behavior. People with Cluster B disorders often struggle to maintain stable relationships, not out of malice, but due to deep-rooted emotional dysregulation and identity confusion.
📊 An estimated 2.8% of the global population lives with a Cluster B personality disorder.
Healthline & DSM-5-TR Note: To be diagnosed with a Cluster B personality disorder:
Symptoms must begin by early adulthood.
If diagnosed before age 18, symptoms must be present for at least one year.
Symptoms should not be attributable to another mental disorder, substance use, or acute stressor.
1. Borderline Personality Disorder (BPD)
Marked by emotional instability, intense relationships, and a deep fear of abandonment. BPD is often misunderstood as “moodiness”, but it goes far deeper - rooted in chronic pain, identity confusion, and attachment trauma.
DSM-5-TR Diagnostic Criteria: (5 or more symptoms)
Desperate efforts to avoid real or imagined abandonment
Unstable, intense relationships swinging between idealization and devaluation
Identity confusion or unstable self-image
Impulsivity in potentially harmful areas (e.g., sex, substance use, reckless spending)
Recurrent suicidal thoughts or self-harming behaviors
Intense emotional reactivity and mood shifts
Chronic feelings of emptiness
Inappropriate or uncontrollable anger
Temporary stress-related paranoia or dissociation
💡 Clinical Insight:
Cleveland Clinic reports BPD often co-occurs with:
Mood disorders (80–96%)
Anxiety (88%)
Substance use (64%)
Eating disorders (53%)
ADHD (10–30%)
Bipolar disorder (15%)
🧬 Risk Factors (as per Mayo Clinic):
Genetic vulnerability
Emotional neglect or abuse in early childhood
Unstable attachments with caregivers
🛠️ Treatment Note: Dialectical Behavior Therapy (DBT) has transformed outcomes for many with BPD, helping develop emotional regulation, distress tolerance, and interpersonal skills.
2. Antisocial Personality Disorder (ASPD)
Defined by a pervasive disregard for others’ rights, manipulation, and lack of remorse. It’s not just “being mean” - it involves chronic patterns of deceit, aggression, and impulsive rule-breaking.
DSM-5-TR Diagnostic Criteria: (3 or more symptoms)
Repeated law-breaking or criminal behavior
Chronic dishonesty or use of aliases for personal gain
Impulsive decision-making or poor planning
Frequent aggression or involvement in fights
Reckless disregard for personal or others’ safety
Irresponsibility in work or financial obligations
Lack of guilt or rationalizing mistreatment of others
🔎 Gender Differences:
Research shows a 3:1 male-to-female ratio, though women with ASPD may present more emotional volatility and higher trauma histories. According to research, they often have less violent but more reactive aggression and are more likely to experience victimization and lack of support.
🧠 Clinical Challenge: People with ASPD rarely seek therapy voluntarily, and often present with charm that masks deeper patterns of manipulation.
Therapists actively engage with patients, families, and interdisciplinary teams to discuss the diagnosis, anticipated course, and management plans for antisocial personality disorder.
3. Histrionic Personality Disorder (HPD)
HPD is characterized by excessive emotionality and attention-seeking. Individuals with this disorder are often perceived as dramatic or flirtatious, but these behaviors are unconscious attempts to gain connenction and reassurance.
DSM-5-TR Diagnostic Criteria: (5 or more symptoms)
Discomfort when not the center of attention
Inappropriate flirtatious or seductive behavior
Rapidly shifting and shallow emotional expressions
Constant use of appearance to gain attention
Style of speech that lacks detail or is impressionistic
Dramatic or exaggerated emotional displays
High suggestibility or easily influenced by others
Misjudging the closeness of relationships
🧬 Comorbidities: Frequently overlaps with narcissistic, borderline, and antisocial traits. HPD is not about manipulation - these behaviors often arise from deep fears of being ignored or unseen.
🧠 Social Insight: Individuals may act theatrically in professional or inappropriate settings without awareness of how it’s perceived.
4. Narcissistic Personality Disorder (NPD)
NPD involves patterns of inflated self-importance, fragile self-esteem, and a constant need for validation. It’s not just arrogance - it’s often a deep vulnerability masked by grandiosity or manipulation.
Treating Narcissistic Personality Disorder is often challenging. Individuals with NPD commonly hold grandiose fantasies and are convinced they deserve special treatment. These characteristics typically emerge by early adulthood and must be consistently evident across various contexts, including professional and personal relationships.
DSM-5-TR Diagnostic Criteria: (5 or more symptoms)
Grandiose view of self and exaggerated achievements
Fantasies of unlimited power, beauty, or success
Belief in being uniquely special or only understood by high-status individuals
Need for excessive admiration
Sense of entitlement or expecting special treatment
Manipulating others for personal gain
Lack of empathy
Envious of others or belief that others envy them
Arrogant, haughty behaviors or attitudes
🧠 Harvard Health notes NPD is 50–75% more common in males, and is associated with elevated risk of depression, social conflict, and even suicide.
🎬 Fictional Illustration: Walter White from Breaking Bad embodies both covert and overt narcissism - swinging between self-righteous justification and emotional cruelty.
💬 Insight: NPD can be covert (insecure, hypersensitive) or overt (dominant, grandiose). Often, people with NPD avoid therapy or present with a “false self” that hides vulnerability.
🧠 Summary: Cluster B in Context
Disorder | Key Feature | DSM-5-TR Criteria Highlights | Character Illustration |
Borderline PD | Instability in mood, identity, and relationships | Fear of abandonment, impulsivity, emotional swings | – |
Antisocial PD | Disregard for rights of others | Lawbreaking, deceit, aggression, lack of remorse | – |
Histrionic PD | Emotionality and attention-seeking | Needs to be center of attention, dramatic behavior | – |
Narcissistic PD | Grandiosity and fragile self-esteem | Entitlement, lack of empathy, need for admiration | Walter White (Breaking Bad) |
⚠️ Reminder: Cluster B traits can be extremely painful for those living with them. They often stem from unresolved emotional wounds, early trauma, or learned survival mechanisms. Accurate diagnosis using DSM-5-TR criteria and trauma-informed therapy can change lives.
Cluster C: Anxious or Fearful Disorders
Cluster C personality disorders are defined by persistent patterns of fear, anxiety, and behavioral avoidance. These individuals often crave connection, stability, or control - but their inner fears can hold them back from relationships, growth, and emotional freedom.
According to mentalhealth.com, a struggle to interact correctly with others and to advance in life often leads individuals with this condition to exist on the fringes of society.
📊 Globally, about 5.0% of the population lives with a Cluster C personality disorder - the highest prevalence among all three clusters.
🧠 DSM-5-TR Note: These traits must be:
Long-standing (starting in early adulthood)
Rigid across personal and professional contexts
Causing significant distress or functional impairment
Not better explained by another mental health condition
1. Avoidant Personality Disorder (AVPD)
Marked by deep feelings of inadequacy, extreme fear of criticism, and chronic social withdrawal - despite a strong desire for closeness. This isn’t just shyness; it’s an inner voice that constantly whispers “you’re not good enough”.
Females could have a somewhat elevated chance of developing the condition.
🧠 DSM-5-TR Diagnostic Criteria (4 or more symptoms):
Avoids social jobs or activities out of fear of criticism or rejection
Withholds from personal connections unless certain of being liked
Holds back in close relationships due to fear of ridicule
Worries obsessively about disapproval or rejection in public spaces
Reluctant to try new social situations out of fear of not being good enough
Sees self as socially inept, inferior, or unappealing
Avoids risks or new ventures that could lead to embarrassment
🧠 Emotional Insight:
While AVPD often appears as “quiet” or “withdrawn”, many individuals yearn for relationships - they’re just afraid they’ll never be accepted.
📚 Origins: Childhood environments with excessive criticism, shame, or conditional affection can increase risk. Parenting styles that emphasized guilt, perfection, or emotional distance are frequently reported.
🎬 Fictional Illustration: Neville Longbottom in Harry Potter exemplifies AVPD traits - timid, self-doubting, and fearful of criticism, yet deeply loyal and capable when given time and trust.
2. Dependent Personality Disorder (DPD)
DPD is characterized by an overwhelming need to be cared for, leading to submissive behaviors and fear of abandonment. People with DPD often feel incapable of making decisions without others’ input.
🧠 DSM-5-TR Diagnostic Criteria (5 or more symptoms):
Needs constant advice or reassurance for everyday decisions
Requires others to take responsibility for major life areas
Fears expressing disagreement in relationships
Avoids initiating tasks due to lack of self-confidence
Will go to uncomfortable lengths to receive support or care
Feels helpless or panicked when alone due to fear of being unable to cope
Desperately seeks another relationship after one ends
Overwhelming fear of being abandoned or left alone
🧠 Behavioral Insight: These individuals aren’t manipulative - they are deeply afraid of abandonment and often feel incapable of standing alone.
📚 Developmental Risks (as per Healthline):
Neglect or abuse in childhood
Overprotective, authoritarian parenting
Long-term toxic or controlling relationships
Family history of anxiety disorders
💬 DPD rarely presents with impulsivity or anger; instead, it often hides behind soft-spokenness, people-pleasing, and fear of disappointing others.
3. Obsessive-Compulsive Personality Disorder (OCPD)
OCPD is not the same as OCD. While OCD is marked by intrusive thoughts and rituals, OCPD is a personality style focused on perfectionism, control, and moral rigidity. People with OCPD often pride themselves on their discipline - but may not recognize how it negatively impacts others.
🧠 DSM-5-TR Diagnostic Criteria (4 or more symptoms):
Preoccupied with rules, details, order, or schedules - even if it ruins the bigger purpose
Perfectionism that blocks task completion
Excessive devotion to work and productivity, ignoring recreation and relationships
Overly rigid or morally inflexible values
Inability to discard old or useless possessions
Hesitates to delegate tasks unless others follow their exact methods
Miserly approach to spending - saves excessively for potential disaster
Displays stubbornness and rigidity in beliefs or routines
🧠 Clinical Difference:
Unlike OCD, individuals with OCPD often do not see their behavior as problematic. They may believe their way is the “right way” and feel frustrated when others don’t live up to their standards.
📚 OCD UK notes: People with OCPD often have little insight into their behavior, while those with OCD usually recognize their thoughts as irrational and seek help.
🎬 Fictional Illustration: Sheldon Cooper in The Big Bang Theory represents OCPD traits - strict routines, intense perfectionism, and low tolerance for deviation, often creating friction in relationships.
🧠 Summary: Cluster C in Context
Disorder | Key Feature | DSM-5-TR Criteria Highlights | Character Illustration |
Avoidant PD | Fear of rejection and inadequacy | Avoids risks, social anxiety, extreme self-criticism | Neville Longbottom (Harry Potter) |
Dependent PD | Excessive need for care | Cannot make decisions alone, fears abandonment | – |
Obsessive-Compulsive PD | Perfectionism and control | Rigid, overly rule-bound, controlling of self and others | Sheldon Cooper (Big Bang Theory) |
⚠️ Reminder: Cluster C disorders are often mistaken for anxiety or introversion. But these patterns are more pervasive, emotionally consuming, and impair daily functioning.
Therapy can help reframe beliefs, increase self-worth, and build healthier relationships.
Spotlight on Narcissistic Personality Disorder (NPD)
Narcissistic Personality Disorder (NPD) is one of the most misunderstood mental health conditions. It’s often associated with arrogance, entitlement, and vanity - but beneath that surface, it can mask a fragile and deeply wounded sense of self.
People with NPD often struggle with chronic feelings of inadequacy, even if they appear confident or successful. Their need for admiration, control, or validation may be rooted in early emotional injuries, shame, or unmet attachment needs.
Overt vs. Covert Narcissism
NPD isn’t always loud.
Overt narcissism is easier to spot - it involves grandiosity, dominance, and visible entitlement.
Covert narcissism, however, is quieter and harder to detect. These individuals may appear sensitive, shy, or anxious, but underneath lies hypersensitivity to rejection, deep envy, and a need for constant reassurance.
Both types can involve intense emotional reactions - including narcissistic rage - when their ego is wounded. This might look like explosive anger, passive-aggressive behavior, or long periods of withdrawal and stonewalling.
In close relationships, this can lead to a painful cycle:
Idealization (love-bombing or putting you on a pedestal)
Devaluation (emotional withdrawal, criticism, or control)
Discard (pulling away or blaming you)
...and then it starts again.
People who live with or care for someone with NPD often describe feeling like they’re walking on eggshells - unsure when the next outburst might come or whether the affection they’re receiving is real.
What Makes NPD Difficult to Spot
Because people with NPD can be charismatic, articulate, or highly successful, they’re often overlooked in clinical settings. Their distress might be masked by charm or defensiveness, making it harder for therapists or even close family members to recognize what’s going on beneath the surface.
That’s why therapy can be especially complex. There’s currently no standardized, manualized therapy for NPD, but Mentalization-Based Treatment (MBT) offers a promising approach. It helps individuals reflect on their internal emotional states and understand how their behavior impacts others - without shame or blame.
The “SPECIAL ME” Framework
Duke Health recommends this acronym to understand the diagnostic picture:
Sense of self-importance
Preoccupied with power, success, or beauty
Entitled
Can only associate with “special” people
Interpersonally exploitative
Arrogant behavior
Lack of empathy
Must be admired constantly
Envious of others (or believes others envy them)
NPD is not about selfishness. It’s about identity, attachment, and fear. And with the right support, healing is possible - even if it’s hard-earned.
Spotlight: Borderline Personality Disorder (BPD)
Borderline Personality Disorder is often reduced to “intense emotions” or “mood swings”, but that framing misses the deeper truth. At its core, BPD is a condition shaped by deep emotional sensitivity, a longing for connection, and an overwhelming fear of abandonment.
Psychology Today suggests a few reasons why someone might develop BPD. It often comes down to a mix of things like your genetics, the chemical makeup of your brain, and tough experiences growing up. This could mean a traumatic childhood with abusive or unpredictable parents. Plus, severe emotional neglect as a child also plays a big part.
People with BPD often feel emotions more acutely than others. Love, rejection, sadness, anger - it all hits harder and lasts longer. When someone they care about pulls away, even briefly, the fear of abandonment can be so intense that it feels unbearable. And in trying to avoid that abandonment, they may act impulsively - even in ways they regret later.
The Pain Behind the Behavior
What’s often seen as “dramatic” or “unstable” is actually a survival strategy. Many individuals with BPD have lived through emotional neglect, trauma, or chaotic caregiving. Their nervous systems were never taught how to trust, regulate, or feel safe in relationships.
This shows up as:
Splitting - seeing people & situations as all good or all bad, shifting rapidly between idealization and disappointment. Splitting can sometimes be done as a defence mechanism.
Impulsivity - reacting without a filter when overwhelmed by emotions
Chronic emptiness - feeling like they don’t know who they really are without external validation
It’s important to note: many people with BPD are deeply empathetic and loving. But the pain of being left - or the idea that they might be - can lead them to push others away before they themselves are pushed.
A Life-Changing Treatment: DBT
Dialectical Behavior Therapy (DBT) has brought tremendous hope for people with BPD. It combines mindfulness with emotion regulation, distress tolerance, and interpersonal effectiveness.
We’ll explore DBT in more detail later, but for now, know this: BPD is not untreatable. With the right therapeutic environment, many people go on to lead grounded, fulfilling, and emotionally rich lives.
How Do You Know If Someone Has a Personality Disorder?
One of the most important - and confusing - aspects of personality disorders is that they’re not always obvious. Many people with personality disorders function well in certain areas of life. They may be high-achieving at work or socially charismatic, but still struggle deeply with relationships, self-worth, or emotional control.
It’s About Patterns, Not Moments
A diagnosis isn’t based on isolated incidents. It’s based on long-standing patterns that show up across settings - in work, friendships, family, or romantic relationships.
According to PsychCentral, two or more of the following areas are usually impacted:
How a person thinks about themselves and others (cognitions)
Emotional range and stability (affect)
Interpersonal relationships
Impulse control
If these issues cause chronic distress or disruption, especially when they’ve been present since adolescence or early adulthood, a personality disorder may be part of the picture.
For Parents and Caregivers
In young people, early signs may include:
Persistent black-and-white thinking (“everyone hates me” vs. “everyone loves me”)
Intense fear of rejection
Ongoing conflicts in friendships
Difficulty managing anger or impulse-driven behavior
But remember - diagnosis is not about labeling. It’s about understanding. And that understanding can only come through a careful clinical process involving:
Structured interviews (like the SCID-5)
Psychological tools (like the Personality Inventory for DSM-5 or PID-5)
A clear history of behavior patterns over time
If someone you love seems to be struggling, compassion - not confrontation - is the first step. Personality disorders don’t define someone’s worth. But naming the problem can be the beginning of healing.
What Causes Personality Disorders?
Personality disorders don’t come out of nowhere. They often develop from a complex mix of genetics, early environment, temperament, and social experiences - all of which shape how we learn to relate to the world and to ourselves.
The American Psychological Association (APA) outlines several contributing factors with key research references:
1. Genetic Predisposition
While there’s no single “personality disorder gene”, research suggests that genetics can influence the development of traits like fear, anxiety, aggression, and emotional sensitivity - which may, in turn, increase vulnerability to personality disorders.
For example, one research team identified a malfunctioning gene linked to obsessive-compulsive traits, while others have explored genetic links to impulsivity and emotional dysregulation, key features in many disorders.
2. Childhood Trauma and Emotional Environment
The Collaborative Longitudinal Personality Disorders Study found a strong connection between childhood trauma and later personality dysfunction.
Borderline personality disorder, in particular, was strongly linked to early experiences of sexual trauma.
Even verbal abuse, such as being frequently yelled at or emotionally rejected by caregivers, was shown to increase the risk of developing borderline, narcissistic, obsessive-compulsive, or paranoid traits in adulthood.
These early experiences disrupt a child’s ability to form secure attachments and to regulate their emotions - key building blocks of personality development.
3. Temperament and Reactivity
Some children are more emotionally sensitive or reactive than others. Known as high reactivity, this temperament makes them more easily overwhelmed by stress, change, or sensory input - which can affect how they relate to others.
According to APA, this kind of biological sensitivity may increase the likelihood of developing shy, withdrawn, or anxious personality styles, especially if paired with an invalidating or unpredictable environment.
4. Protective Social Factors
Not all children exposed to adversity develop personality disorders. The APA notes that positive relationships - with a caregiver, teacher, or even a single friend - can offset negative influences and build emotional resilience.
Addition: Neurobiology and Brain Structure
Structural and functional differences in the brain are also implicated.
Neuroimaging studies have identified abnormalities in areas related to emotion regulation, impulse control, and social cognition, especially in people with borderline personality disorder (BPD):
Reduced gray matter in regions like the amygdala, hippocampus, ventral cingulate gyrus, and orbitofrontal cortex
Differences based on sex: BPD women tend to show reduced volume in the medial temporal lobe, while BPD men show more changes in the anterior cingulate cortex
These changes aren’t the sole cause of personality disorders, but they may amplify emotional sensitivity, impulsivity, and relational difficulties - especially when combined with environmental stress.
How Personality Disorders Affect Life
Personality disorders are often invisible from the outside - but for the person living with one, the impact touches nearly every part of daily life. From relationships to self-worth, the effects are chronic, deep-rooted, and emotionally exhausting.
1. Relationships
Many people with personality disorders want close, stable relationships - but may find themselves stuck in patterns of:
Fear of abandonment or rejection
Overdependence or emotional detachment
Explosive conflict or emotional withdrawal
What starts as love or connection can quickly spiral into mistrust, insecurity, or misunderstanding.
2. Work and Career
At work, challenges may include:
Difficulty accepting feedback or criticism
Struggles with authority, rigid rules, or collaboration
Emotional dysregulation that leads to burnout, frequent job changes, or underperformance
Even highly capable individuals may self-sabotage or feel chronically “not good enough”.
3. Self-Image and Identity
Living with a personality disorder can feel like never really knowing who you are. Common issues include:
Shame, self-hatred, or deep-seated feelings of inadequacy
Difficulty maintaining a stable sense of self
Constant self-doubt and fear of how others perceive you
4. Mental Health Struggles
Personality disorders often co-occur with other mental health conditions like:
Depression
Anxiety
Substance use
Eating disorders
PTSD or trauma-related disorders
Without integrated care, these conditions can intensify each other, making recovery harder.
5. Suicide Risk
Because of the intense emotional pain and impulsivity involved, people with certain personality disorders - particularly borderline personality disorder - are at higher risk for self-harm and suicide.
This makes early recognition, compassion, and professional intervention all the more critical.
Substance Use and Co-Occurring Disorders
Personality disorders rarely show up in isolation. Most individuals experience co-occurring disorders, especially when it comes to substance use.
According to the US National Institute of Mental Health (NIMH):
Around 22.6% of people with any personality disorder also have a substance use disorder (SUD)
Among those with BPD, this rate jumps to 38.2%
Other studies report:
83% of individuals with BPD have a mood disorder
85% have an anxiety disorder
53% meet criteria for another personality disorder
10–20% have bipolar I or II disorder
Why Does This Happen?
For many, substances like alcohol, cannabis, or stimulants become a way to manage emotional pain, numb feelings of emptiness, or feel “in control”.
However, substance use can worsen emotional regulation, increase impulsivity, and make therapy less effective - leading to a cycle that’s hard to break.
People with Cluster B disorders, in particular, face an increased risk of suicidal ideation, which becomes even more dangerous when substance use is involved.
If Left Untreated
When personality disorders go unrecognized or untreated, the long-term impact can be profound. These are not just “difficult personalities” - they’re mental health conditions that shape every aspect of life.
1. Chronic Emotional Pain
Without treatment, many individuals experience:
Lifelong patterns of distress, emptiness, or rage
Repeated feelings of failure or unworthiness
Cycles of conflict, isolation, and disconnection
2. Risk of Harm
Untreated personality disorders are linked to:
Higher rates of self-harm
Increased suicide attempts
More frequent use of substances to cope
3. Relationship and Parenting Difficulties
Struggles with emotional regulation and trust can make it hard to:
Parent consistently or set healthy boundaries
Maintain long-term partnerships
Build mutual respect in relationships
4. Stalled Personal Growth
Many individuals find it difficult to:
Stay in school or hold down jobs
Trust therapists or stick with treatment
Set and achieve long-term goals
But none of this is inevitable. With compassionate care and the right therapeutic approach, personality disorders can be treated - and people can lead meaningful, connected, and fulfilling lives.
Treatment That Works
Personality disorders aren’t character flaws - they’re deeply rooted patterns of thinking, feeling, and relating that often begin in childhood and become harder to shift over time. That’s why treatment is possible, but it takes time, patience, and the right support system.
Therapy is the cornerstone. Medications may help with specific symptoms, but meaningful change typically happens in the context of a stable therapeutic relationship, where emotional patterns can be gently understood and transformed.
Dialectical Behavior Therapy (DBT): Especially Effective for BPD
Originally developed for borderline personality disorder, DBT has become one of the most evidence-based treatments for helping people manage emotional intensity, self-destructive behaviors, and relationship struggles.
What sets DBT apart is its balance between acceptance and change. It doesn’t just teach you how to stop destructive behaviors - it helps you understand where they come from.
DBT helps build four essential skills:
Mindfulness: Being present without judgment
Distress Tolerance: Surviving crisis moments without making things worse
Emotion Regulation: Naming, understanding, and managing big feelings
Interpersonal Effectiveness: Learning to ask for what you need while maintaining self-respect and relationships
People with BPD often describe DBT as life-changing. For many, it’s the first time they learn how to sit with overwhelming emotions - instead of being ruled by them.
CBT, Schema, and Psychodynamic Therapies
While DBT is a great fit for BPD, other therapies are helpful for different personality disorders:
Cognitive Behavioral Therapy (CBT) focuses on reframing distorted thinking patterns and building healthier behaviors.
Schema Therapy blends CBT with emotional healing. It explores how early unmet needs can create lifelong “schemas” - like feeling unlovable or defective - and helps individuals rewrite those narratives.
Psychoanalytic or Psychodynamic Therapy looks at unconscious patterns and how early relationships shaped the self. These longer-term approaches can help people gain deep insight into why they relate the way they do - and begin to do it differently.
Medication: Helpful, But Not a Cure
According to Mind UK, there are no medications specifically designed for personality disorders. However, doctors may prescribe:
Antidepressants (for persistent sadness or hopelessness)
Mood stabilizers (for intense mood swings or irritability)
Antipsychotics (for paranoia or severe disorganization)
These are usually prescribed for co-occurring conditions like depression or anxiety, rather than the core personality traits themselves.
Support During Life Transitions
People with personality disorders often need additional support during major life transitions, such as:
Pregnancy and parenting
Grief or relationship endings
Job loss or retirement
Moving out of the family home
These changes can unearth old fears or destabilize coping strategies. Therapy during these periods isn’t just helpful - it can be essential for maintaining progress and emotional safety.
Can Personality Disorders Be Prevented?
We often think of personality disorders as something that “just happens” in adulthood - but the roots are almost always laid down early. That’s why early prevention, especially emotional attunement in childhood, can make a lasting difference.
“Borderline personality disorder may be the most preventable of all mental illnesses.”
- Interpreted from Dr. Andrew Chanen’s work, 2013
While most prevention research has focused on BPD, the principles apply broadly: supportive environments, secure attachments, and emotional literacy reduce risk - and help children grow into emotionally resilient adults.
What Helps?
1. Emotionally Attuned Caregiving
Children who feel seen, soothed, and supported are more likely to develop a stable sense of self and trust in others.
They learn that:
Feelings are valid
Mistakes don’t mean rejection
Relationships can survive conflict
This kind of caregiving helps prevent the shame, fear, and identity confusion often seen in personality disorders later in life.
2. Secure Attachment and Role Models
Caregivers who model healthy emotional expression - naming their feelings, calming themselves, repairing conflict - give children a roadmap for handling their own emotions and relationships.
Even one safe adult, whether a parent, teacher, or relative, can become a buffer against early trauma or neglect.
3. Emotionally Healthy School and Community Environments
Prevention also goes beyond the home. Schools that teach emotional intelligence, empathy, and communication skills can give children the tools to navigate conflict, set boundaries, and handle rejection - key protective factors.
Communities that reduce stigma and promote access to early mental health care can also help identify and address problems before they solidify into personality patterns.
A Final Word on Prevention
Not every personality disorder can be prevented. Genetics, temperament, and life experiences all play a role. But creating emotionally nurturing environments - at home, in school, and in society - can significantly lower risk.
And for those already struggling: it’s never too late to heal. Prevention matters. But so does compassion, support, and therapy at any age.
How Elfina Can Help
At Elfina, we believe that therapy should feel like being truly seen - not judged.
Living with a personality disorder can often mean carrying years of pain, shame, or confusion. Many people feel misunderstood, dismissed, or afraid to reach out. That’s why we’ve built a therapy experience that prioritizes trust, cultural sensitivity, and deep emotional safety.
Here’s what makes Elfina different:
🎯 94% therapist-client match on the very first try
Because healing starts with the right person.👩⚕️ 80%+ of our therapists have 5+ years of experience
We work with specialists who understand complex trauma, personality patterns, and the emotional depth behind the diagnosis.🧘 Culturally aware and trauma-informed care
Our therapists understand the unique emotional landscapes shaped by family, culture, and societal expectations - especially in South Asian and Indian contexts.🔒 Judgment-free, confidential spaces for long-term healing
Whether you're struggling with identity, fear of abandonment, emotional regulation, or just trying to understand why relationships feel so difficult - you don’t have to face it alone.
At Elfina, we don’t rush you. We meet you where you are, at your pace, with compassion and clinical care. Because therapy isn’t just about managing symptoms - it’s about rebuilding your relationship with yourself.
Conclusion: This Is Not the End - It’s a Beginning
A personality disorder is not a brokenness.
It’s not a failure of character.
And it’s certainly not something to be ashamed of.
It’s a way of describing deeply persistent emotional patterns — ones that were often shaped by early wounds, unmet needs, or survival strategies that no longer serve us.
But with therapy, support, and self-compassion, these patterns can change.
People with personality disorders can and do:
Build stable, loving relationships
Create meaningful careers
Learn to feel safe in their own emotions
Reconnect with joy, purpose, and peace
It’s not easy. Healing takes time. But it is absolutely possible.
At Elfina, we’re honored to walk that path with you - step by step, with the respect and care you deserve. 💙
Other blogs

Frequently Asked Questions
What types of therapy do you offer?
Can I meet my therapist in-person?
How do you match me with a therapist?
How much does therapy cost?
Do you offer free trials?
Finding The Right Fit, Made Easy





© Mindaro Health Technologies. All rights reserved
© Mindaro Health Technologies. All rights reserved
Finding the right fit, made easy.
FAQs
What types of therapy do you offer?
Can I meet my therapist in-person?
How do you match me with a therapist?
How much does therapy cost?
Do you offer free trials?